

A. Introduction
1. Intestinal obstruction은 Mechanical obstruction 또는 adynamic(paralytic) ileus에 의해 food와 bowel content의 passage가 일어나지 않게 된다.
2. Mechanical obstruction의 경우 일반적으로 morbidity와 mortality를 최소화하기 위해 짧은 시간 내에 intervention이 필요함.
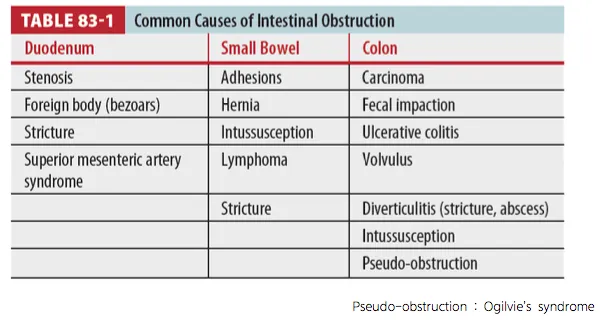
3. Large & small bowel obstruction은 다양한 pathologic process에 의해 발생
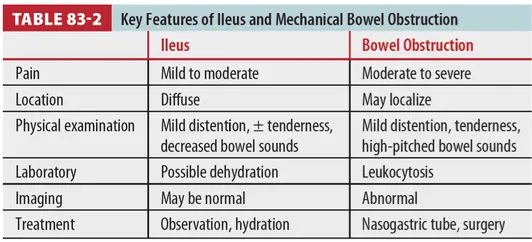
4. Ileus와 bowel obstruction의 특징
B. Pathophysiology
* Bowel obstruction → Bowel congestion & intestinal content absorption 저하
→ Vomiting, poor oral intake → Volume depletion
→ Hemoconcentration, Eletrolytes imbalance → Renal failure, Shock
* Mechanical obstruction → Bowel distension → Intraluminal fluid accumulation
→ Intraluminal pr. 증가 + enhanced peristalic contraction & air swallowing
→ Intraluminal pr.가 bowel wall의 capillary & venous pr. 초과
→ Absorption, lymphatic drainage 감소 → Ischemia, septicemia, bowel necrosis → Shock
* Closed-loop obstruction에서는 위와 같은 단계가 빠르게 일어남.
(예 : Incarcerated hernia, Complete colon obstruction in the presence of a closed IC valve)
B1. Small bowel obstruction의 원인
(1) Small bowel obstruction : most bowel obstructions을 차지
(2) 복부 수술 후 adhesion : m/c
보통 수술 후 수개월에서 수년 후에 발생하나 몇 주만에 발생하는 경우도 있음)
(3) Incarceration of hernia : 2nd m/c
(in elderly, adhesion and hernia still common cause of SBO)
(4) Bariatric surgery : Roux-en-Y gastric bypass 후 internal hernia 발생할 수 있음.
(5) 드문 기타 원인들 (intraluminal or intramural processes)
1 Polyps, lymphoma, adenocarcinoma
2 Peutz-Jeghers syndrome : Hamartomatous polyp, 연령 : 10~30대
3 Gallstone ileus : Eroded gall stone이 IC valve를 막음.
: Sign : pneumobilia + bowel obstruction
(6) Lymphoma : Intussception (leading point 역할을 함)
(7) GI pyloroplasty or pyloric resection을 받은 환자가 bezoar(comfosed of vegetable matter or
pulp)에 의해 intraluminal obstruction이 잘 생김
(8) IBD, abscess, radiation enteritis, Traumatic duodenal hematoma (child, lap belt injury)
(9) Capsule endoscopy의 complication (1%~20%)
B2. Large bowel obstruction의 원인
(1) Neoplasm : m/c (특히 고령, 40대 미만에서도 발병률 증가 추세)
(2) Hernia, surgical adhesion : 거의 일어나지 않음.
(3) Diverticulitis : Mesenteric edema, Stricture
(4) Fecal impaction
: Anticholinergic medication을 용하면서 Elderly, bedridden, psychiatric 환자가 고위험군이고
병력 상 Constipation가 있는 경우가 많음
(6) Cecal volvulus : 임신한 여성에서 위험성이 높음
C. Clinical features
1. History
(1) 거의 모든 환자들이 통을 호소함
(2) 일반적으로 통증은 crampy & intermittent
(3) Pain of mechanical SBO : episodic, 수 분간 지속, periumbilical or diffuse
(4) Adynamic ileus에서는 통증이 less intense, more constant
(5) Proximal obstruction : Bilious vomitus
(6) Distal ileal or LB obstruction : Feculent
(7) Large bowel obstruction의 pain : 일반적으로 하 부에 위치(hypogastric)
(8) Constipation이 일반적 증상 / partial bowel obstruction에서는 변과 가스의 통과
(9) Additional risk factors
1 Advanced age
2 Bowel motility를 감소시키는 anticholinergic, tricyclic antidepressants
2. Physical exam
(1) Distension : SBO - reliable sign
(2) Tenderness : Minimal ~ severe, localized or diffuse
(3) Peritonitis : Severe pain
(4) Percussion : Tympanic
(5) Mechanical obstruction
: High-pitched bowel sound - 진행되면 peristaltic wave와 bowel sound가 감소
(6) Adynamic ileus : Abd. distension + Bowel sound 감소
(7) Localized or rebound tenderness
: Gangreneous or perforated - immediate surgical intervention
(8) Sigmoid volvulus : Simple film 상 Emptiness of the left iliac fossa - reliable sign
(9) Organomegaly, Mass : Obstruction의 원인
(10) Rectal vault 내의 absence of stool or air : Obstruction 진단에 도움
(11) Rectal vault 내의 presence of stool or air : Not eliminate a more proximal obstruction.
(12) Rectal exam : Fecal impaction, rectal carcinoma, occult blood, stricture를 확인
(13) Pelvic exam : Vaginal pessary 유무 확인 (Colon compression을 유발할 수 있음)
D1. Diagnosis
부 통증과 팽만이 있는 모든 환자에게서 bowel obstruction or ileus를 고려할 것!
D1. Lab
(1) CBC, eletrolyte
(2) WBC>20000 or Lt. shift : bowel gangrene, intra-abdominal abscess, peritonitis를 가능성
(3) Amylase, Lipase : 약간 상승
(4) WBC>40000 : mesenteric vascular occlusion 가능성
(5) Hematocrit, BUN, creatinine 상승 : Volume depletion, dehydration을 의미
(6) Urine specific gravity, ketonuria, lactate 상승, metabolic acidosis
: Obstruction severity의 또 다른 지표
(7) Procalcitonin : Bowel ischemia와 management failure의 predictor
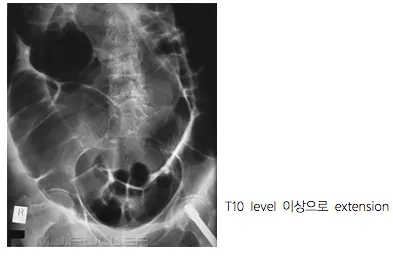
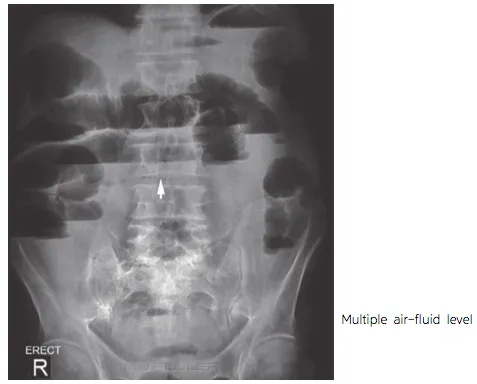
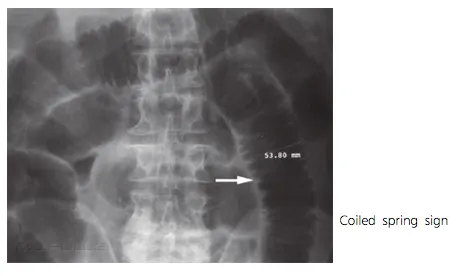
D2. Imaging
(1) Simple film : Abd S/E, Chest PA, Lat. decubitus (greatest volue : free air detection)
(2) CT scan c contrast (oral or IV) : Imaging method of choice
(3) Renal insufficiency, Contrast allergy : Oral contrast CT rec.
E. Treatment
* SB : 거의 수술 필요 없음 / LB : 대부분 수술이 필요
1. Tumor로 인한 colonic obstruction
(1) Tumor resection이 gold standard
(2) Stent로 응급수술을 피할 수 있음.
2. NG tube는 통 필요하지 않지만 severe distension, vomiting 시 고려해야 함.
3. Vigorous IV fluid replacement가 필요함. : BP, HR, Urine output으로 모니터링
4. Closed-loop obstruction, bowel necrosis, cecal volvulus : Surgical emergency
5. ED에서 preoperative broad-spectrum antibiotics를 사용해야 함.
ex) Monotherapy : Tazobactam-piperacillin, 3.375g IV every 6 hours
또는 Ticarcilin-clavulanate, 3.1g IV every 6 hours 또는 Carbapenem
6. Adynamic ileus : IV fluid, observation, bowel motility 억제시키는 약 stop
Polybutine 100 mg Tab 2T 3P
Gasmotin tab 5mg 1T 3P
Rmanos 250 mg cap 1C 3P
FORLAX Powder 10g/P 1 PKG 2P
5DS 1L + MVH 1A + Nexium 1A 하루 2회
