

•
Large bowel obstruction, occurs when the sigmoid colon twists on its mesentery, the sigmoid mesocolon
•
5% of large bowel obstruction in developed countries, and 10~50% in developing countries
•
Risk factor:
Chronic constipation and/or laxative abuse
Fiber-rich diet
Redundant colon
Medication from chronic psychiatric conditions
A. Clinical presentation
•
Abdominal pain (initially left-sided, later diffuse)
•
Enormous abdominal distension
•
Constipation
•
Nausea & vomiting
B. Diagnosis
B1. Abdomen CT
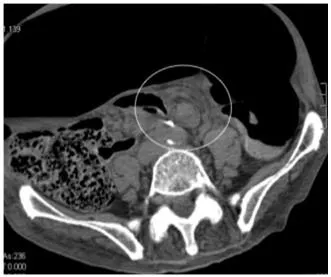
•
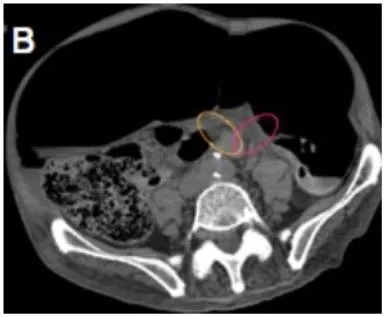
Whirl pattern, caused by the dilated sigmoid colon around its mesocolon & vessels
•
Bird-beak appearance of the afferent and efferent colonic segments
⇒ may absent in one-fourth of CT scans
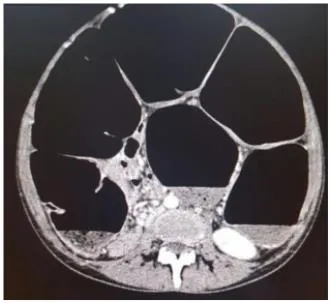
•
Large gas-filled loop lacking haustra, forming closed-loop obstruction
•
Whirl sign
•
Bird beak sign
•
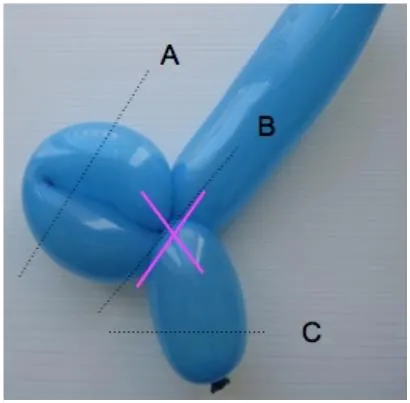
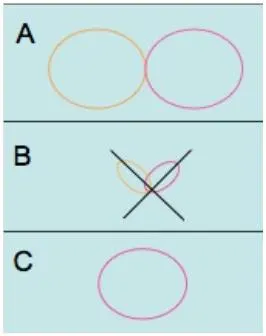
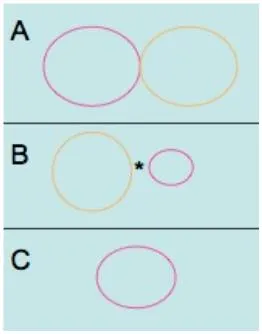
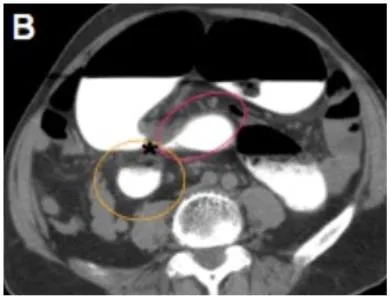
X-marks-the-spot sign : complete obstruction 되면서 distal, proximal sigmoid colon이 둘 다 obstruction 되는데, 이 두 속의 transition point가 반대로 나타나서 마치 x표시 같다.
•
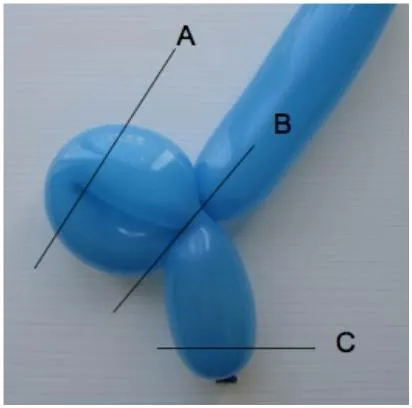
Split wall sign : incomplete obstruction, partial obstruction시 distal, proximal colon 사이 mesenteric fat이 들어가며 마치 둘을 분리시키는 것 같다
•
Steel pan sign


B2. Abdomen X-ray
•
U-shaped, distended sigmoid colon, a haustral collection of gas
⇒ extending from the pelvis to the right upper quadrant
•
Only 60% of patients
B3. Contrast enema
•
bird’s beak configuration
C. Treatment
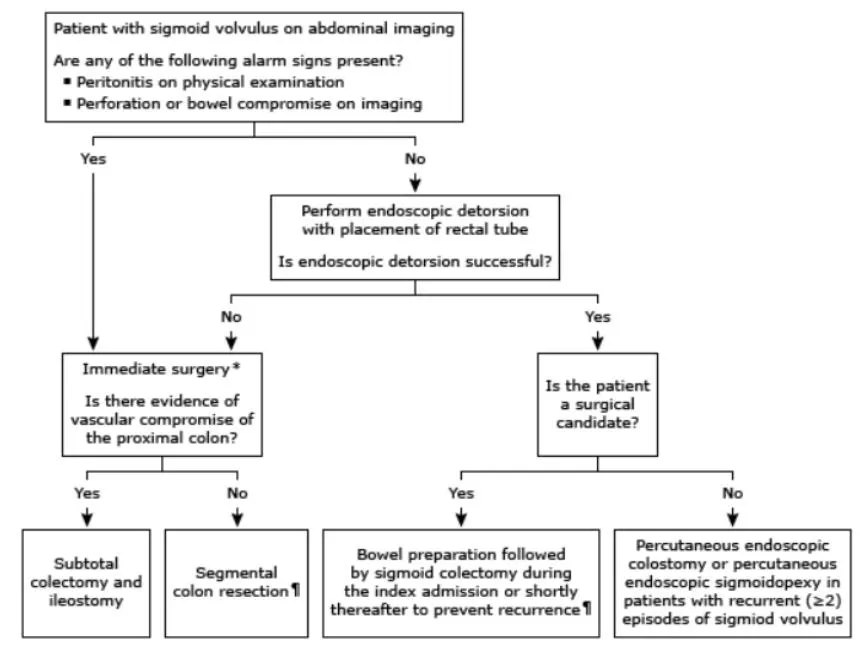
•
Peritonitis 의심소견, 천공 의심소견 ⇒ 응급수술
•
위 사항 없으면 내시경으로 detorsion 시도.
•
Conservative treatment
◦
Rigid/Flexible sigmoidoscopy – decompress proximal bowel
◦
Recurrence: wide range (20~84%)
◦
Failure ⇒ urgent surgical management
