

A. Introduction and epidemiology
A1. EM에서의 management
•
통증 조절
•
신장 기능에 대한 평가
•
Spontaneous stone passage 가능할지 판단
A2. Prevalence
•
5.2% (1994년) → 8.8%(2010년)
•
남자 10.6%, 여자 7.1%.
•
유럽과 동남아에서 증가추세
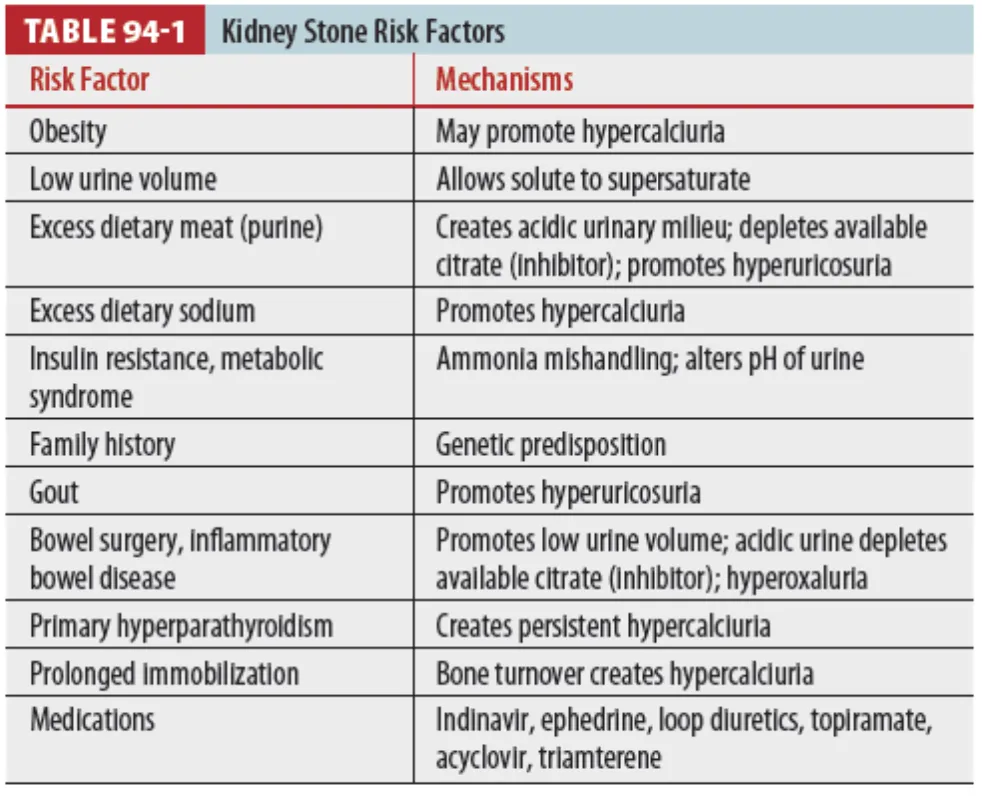
A3. 위험인자
•
비만과 당뇨
A4. 첫 발생 후 재발
•
11%(2년), 20%(5년). 31%(10년), 39%(15년)
B. Pathophysiology
B1. Stone formation
•
Supersaturation : 용해된 salts가 urine을 supersaturate 하여 solid phase로 농축
•
용매인 urine의 양이 많거나 용질인 uric acid, calcium의 양이 적으면 예방에 도움
•
Inhibitory substance (citrate, magnesium) : Crystal의 침전과 stone 형성을 억제
(1) 칼슘석 (Calcium oxalate, Calcium phosphate) : 80% 가량
(2) Struvite (magnesium-ammonium-phosphate) 10% 가량
•
재발하는 UTI.
•
Urea-splitting bacteria 감염과 연관
•
Staghorn calculi.의 가장 흔한 원인
•
Proteus, Klebsiella, Staphylococcus species, Providencia, Corynebacterium
(3) Uric acid (radiolucent) : 10% 가량
•
남자, 통풍, Chemotherapy
B2. Pain
•
Obstruction of a hollow viscus orgarn (Ureter)
•
수신증 및 Gerota's fascia에 지속적인 압력이 가해짐 → Flank pain
•
Isolated small renal pelvis stones은 통증 유발하지 않음
B3. Acute obstruction
•
대부분은 serum creatinine 상승 보이지 않음.
•
반대 콩팥이 최대 185% 까지 기능을 함.
B4. Spontaneous stone passage의 probability를 결정하는 요인들
(1) 크기, 모양, 위치 및 요관 폐색의 정도
(2) Obstruction의 흔한 부위
•
UPJ : 1 cm 정도의 renal pelvis가 2~3 mm 정도의 ureter로 좁아지는 구간
•
Pelvic brim : Ureter course over pelvis and iliac vessels
•
UVJ (most constricted site) : Muscular coat of bladder
(3) Based on stone size alone
•
Diameters < 5mm : 98%에서 4주 이내 자연 배출
•
Diameters 5~7mm : 60%에서 4주 이내 자연 배출
•
Diameters > 7mm : 39%에서 4주 이내 자연 배출
•
Stone size on plain radiographs is magnified by up to 20%
•
measured stone on CT is 88% of actual stone size
C. Clinical features
•
Groin으로 방사되는 acute onset의 crampy intermittent flank pain
•
Rebound td(29%), guarding (61%), rigidity(8%) / Nausea and Vomiting(50%)
•
Renal colic 있는 환자의 85% 만 hematuria 나온다. 30%는 gross hematuria
•
Stone의 위치와 통증 위치 correlation
•
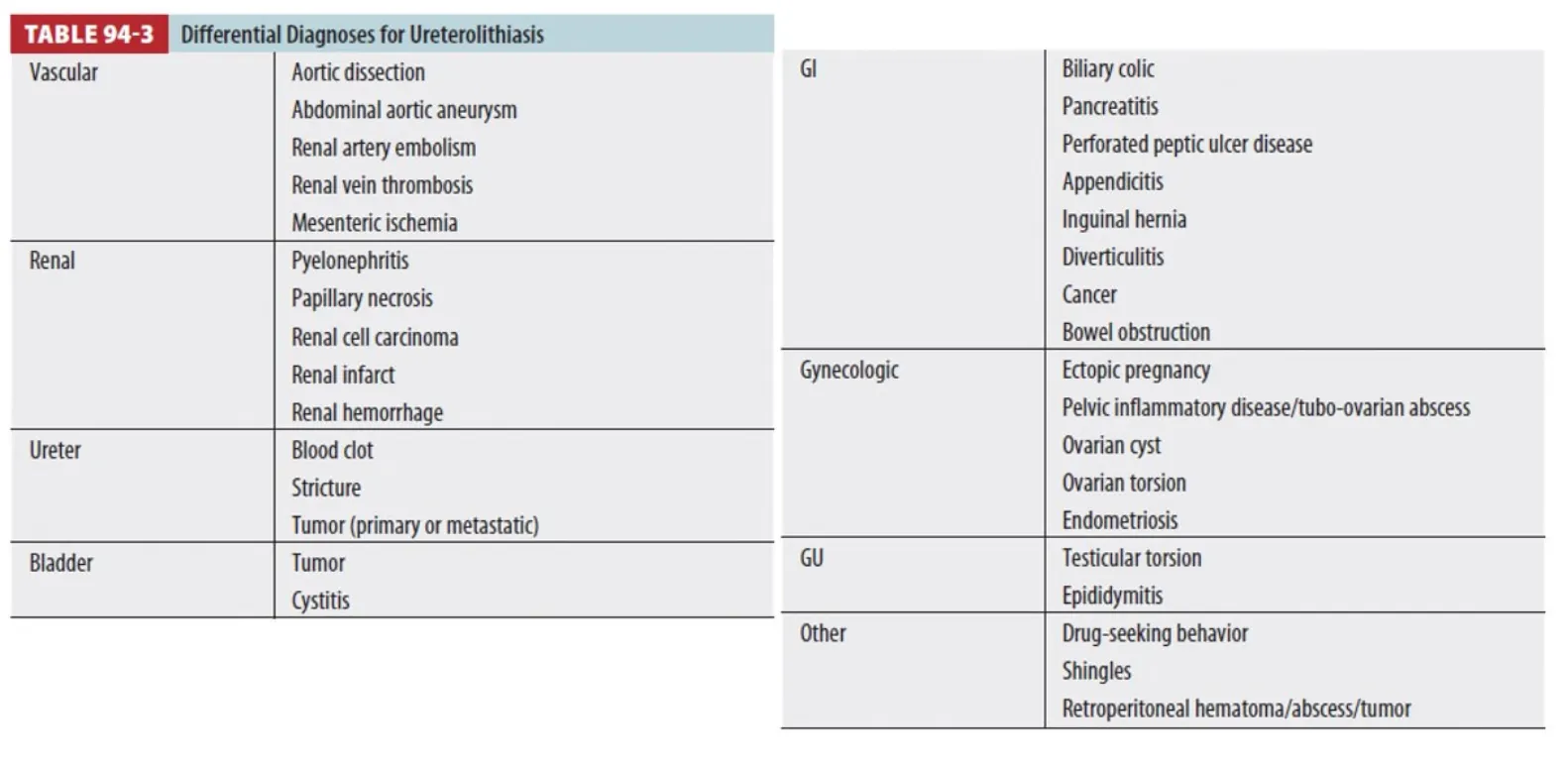
AAA의 파열이나 확장의 가장 흔한 오진 → Nephrolithiasis
D. Diagnosis
D1. Laboratory evaluation
•
감염, 신기능 이상, 임신 가능성 확인 (ectopic pregnancy 가능성).
•
Urinalysis : Infection 배제하기 위해 / 감염 확인되면 urine culture 하기.
•
Hematuria는 없을 수도 있음. (10-15%)
•
Flank pain과 hematuria가 있는 환자의 24%에서는 stone의 영상학적 증거가 없음.
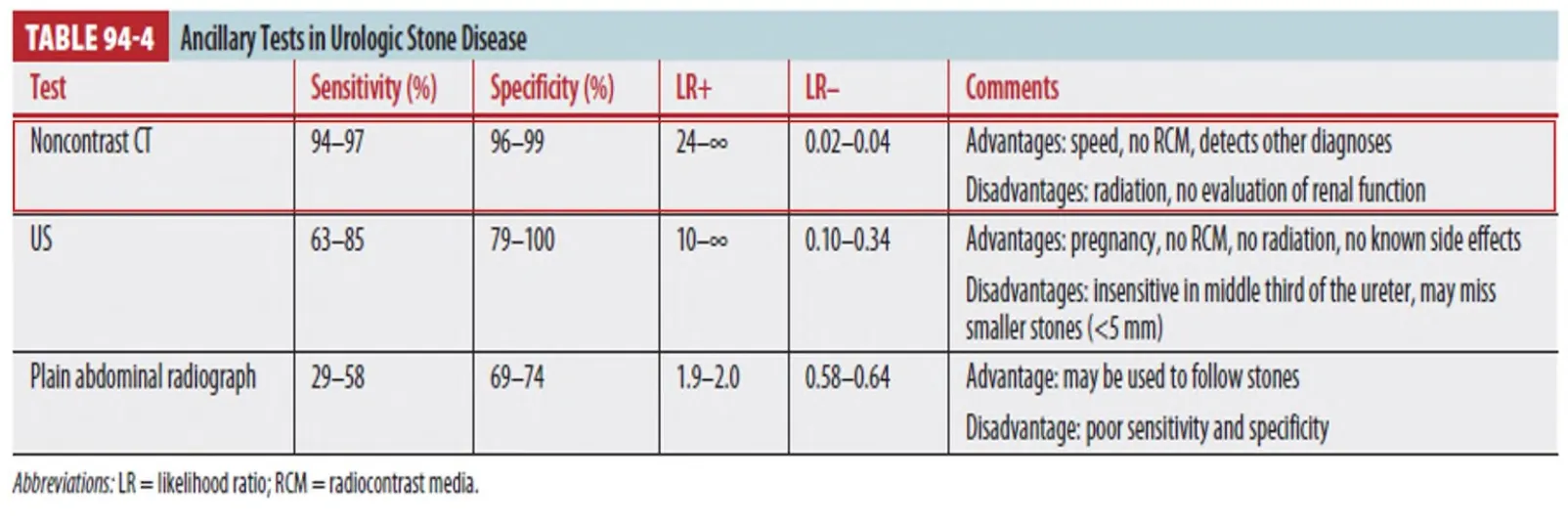
D2. Imaging
E. Treatment
•
Forced hydration 은 효과 없음.
E1. Pain & Nausea/vomiting control
•
NSAIDs, Opioids, Lidocaine + Antiemetics
E2. Antibiotics
•
감염의 증거가 있는 경우
•
Piperacillin-tazobactam, Cefepime, Ticarcillin-clavulanic acid or Ciprofloxacin
•
Without renal compromise : Gentamicin, Tobramycin plus Ampicillin
E3. Medical expulsion theray
•
α-Blockers (tamsulosin) : Expulsion rate 증가시키고 expulsion time 감소시키며 pain을 감소.
•
Surgical intervention rate 는 변화 없음
F. Disposition and Follow up
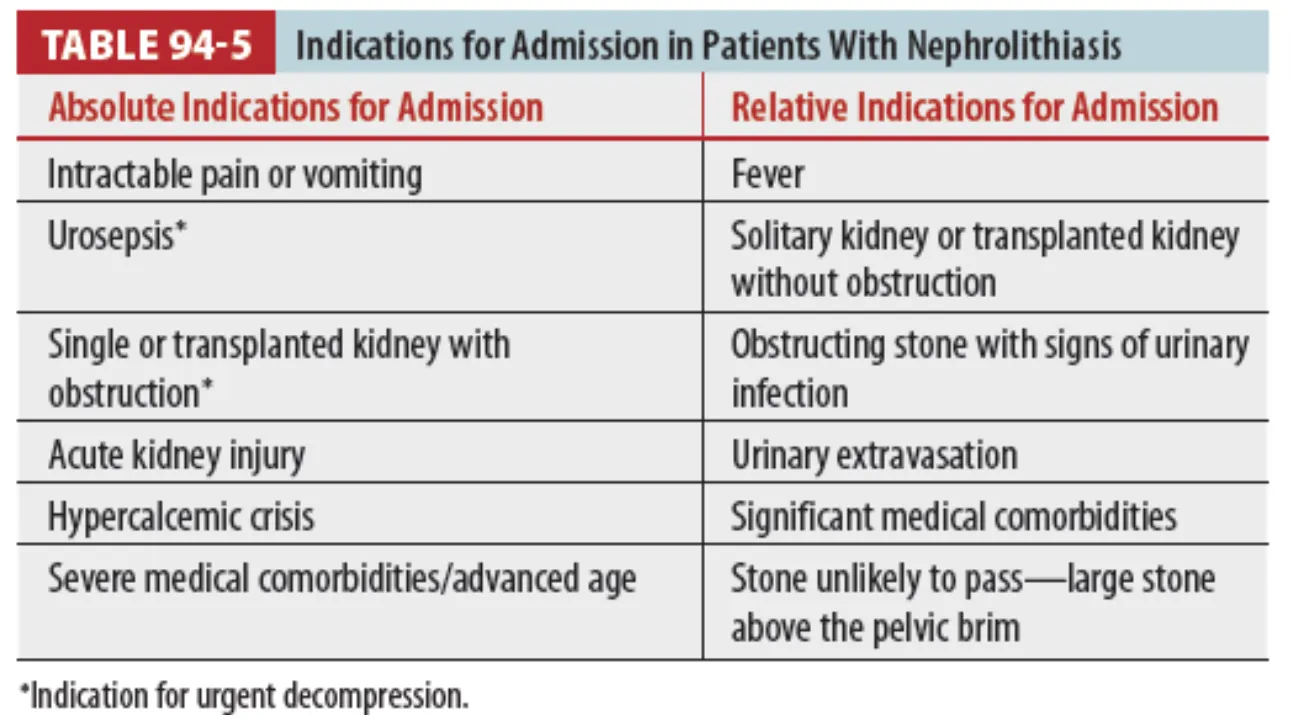
F1. Discharge
•
5mm 이하 작은 크기
•
Infection 없음
•
Oral analgesics로 통증 조절
•
Stone passage time은 크기와 위치에 따라 다양
◦
5~6mm 크기 경우 7일에서 30일정도
