
개요
•
Epilepsy는 오진율이 높다 (20~30% 정도)
•
Convulsion : 불수의적 근육의 움직임
•
Epileptic seizure : 뇌의 비정상적인 활동에 의해 그게 관여하는 기능에 영향 - 매우 다양한 형태로 표현 : 의식, 감각, 운동, 언어 등등
•
Epilepsy : Epileptic seizure 가 24시간 이상의 간격으로 2회 이상 반복.
1번 했어도 재발 가능성이 60% 이상으로 판단된다면 진단가능
첫 seizure 시 epileptic SD에 합당한 경우
A. Pathophysiology
A1. Seizures : Primary (unprovoked) or Secondary (provoked)
(1) Primary seizures 원인
Idiopathic or congenital developmental abnormalities, in utero CNS insult
(2) Secondary seizures 원인
Trauma or Injury / Infection / Metabolic abnormalities (e.g., hypoglycemia, electrolyte abnormalities, inborn errors of metabolism) / Toxins / Systemic illness
B. Clinical features
B1. Types of seizure
(1) Seizure activity is localized (focal) or widespread (generalized)
① Generalized seizures
: Convulsive generalized seizures or grand mal seizures (rhythmic motor activity affects both sides of the body)
: Nonconvulsive generalized seizures (LOC without motor activity, EEG ) 꼭 필요
: Absence seizures (Brief episode of staring without a postictal state)
: Atonic seizures (Sudden loss of muscle tone with a sudden “drop” to the floor)
: Myoclonic seizures
② Partial seizures
: Focal neuronal activity, and clinical features correlate with the affected area
: Simple partial seizures - Remains awake
vs Complex partial seizures - focal but alterations of consciousness
③ Status epilepticus
: Any “prolonged” seizure or recurrent seizures lasting >5 minutes without return to full consciousness
: Nonconvulsive status epilepticus(NCSE) may present as a prolonged postictal state and must be considered in any patient with altered mental status
B2. History
(1) 환아의 연령이 잠재적인 원인 추정에 중요하다
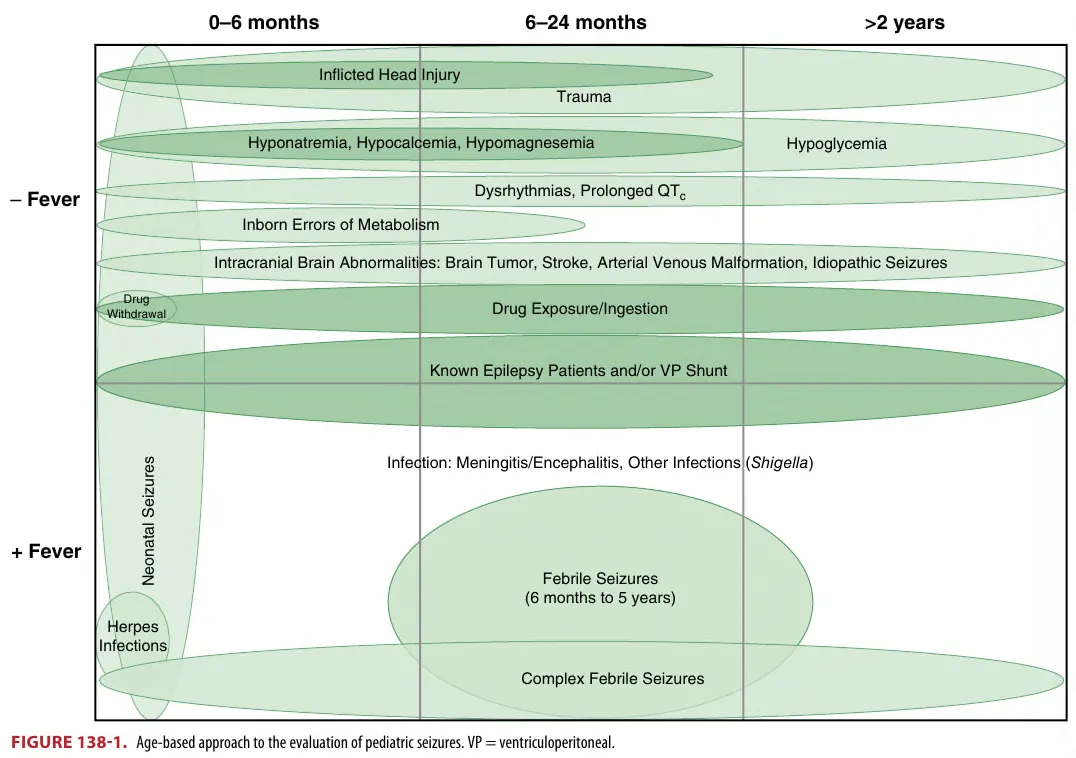

(Fig. 138-1)
B3. Physical exam
•
Head-to-toe examination
•
Focused on whether the patient is actively seizing and identify potential causative factors
(e.g., head trauma, rash indicative of infection, neurocutaneous lesions).
•
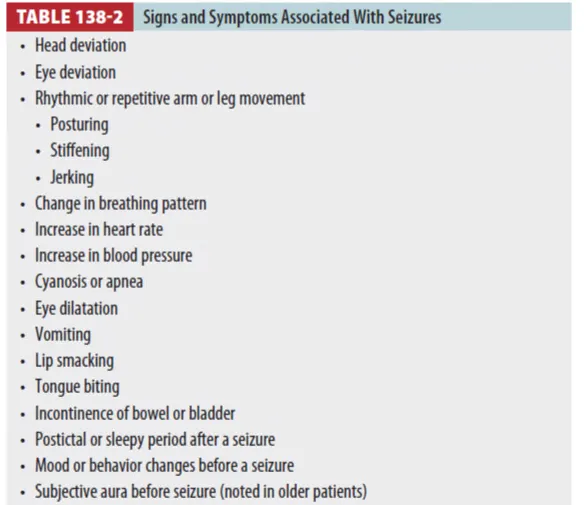
Signs and Symptoms Associated With Seizures (Table 138-2)
C. Diagnosis
C1. Differential diagnosis (Table 138-3)
DDx
(1) Syncope : 경련으로 가장 많이 오진되는 것
•
no postictal state
vs Seizure : associated with tongue biting, rhythmic motor activity, incontinence, and a slow
recovery and postictal state
Syncope와 Seizure 감별 (94%민감도/특이도) : 점수가 1점 이상이면 seizure, 1점 미만이면 syncope
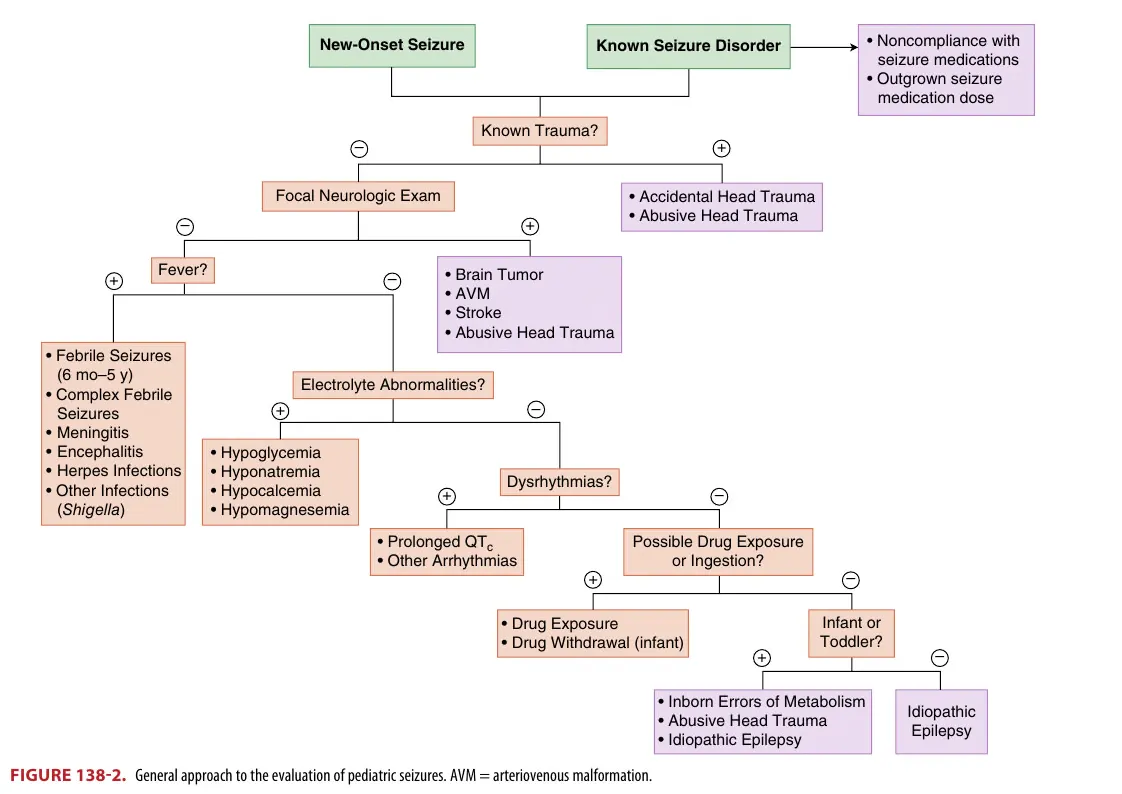
D. Summary of approach to evaluation
E. Treatment
E1. Prehospital
(1) 안전한 환경 만들기
•
똑바로 눕힌다
•
머리에 푹신한 쿠션을 만들어 준다 (+ 옷 풀어주기)
•
주위의 위험한 물건 치운다
•
시간 체크
(2) 경련하는 동안 하지 말 것들
•
입을 억지로 열지 말 것, 물이나 약 주지 말 것
•
혀 깨무는 것을 막으려고 아무것도 넣지 말 것 (특히 손가락이나 잘리는 물체)
•
경련을 손으로 억제하려 하지 말 것
•
5분 이상 경련하면 119 신고
(3) 경련이 끝나면
•
옆으로 눕혀준다 (회복자세)
•
머리를 부드럽게 젖힐 것
E2. 병원 단계 치료
(1) 교과서적으로 5분 이상 지속되면 약물투여
•
대부분의 경련은 5분 이내 멈춘다
•
응급실에 경련하면서 내원한 경우 약물투여
•
의식 회복 없이 경련 반복 시 약물투여 (status임)
•
경련중첩의 경우는 조기에 약물 치료할 때 효과가 더 좋다.
<Benzodiazepines>
- 0.1 mg/kg (max : 2~4 mg)
- BDZ 효과는 발작 기간과 반비례하며 치료가 지연되어서는 안됨
- 최대 2번 까지 (이후로는 효과 떨어지고 부작용만 증가)
- Route : Efficacy 다르지 않으므로 여러 route 사용가능
: IN midazolam : 0,2 mg/kg (max: 10mg) - MAD 필요, onset 이 가장 빠름
: Buccal midazolam : 0.5 mg/kg (max: 10mg) - 농축 mida (15mg/3mL) 가 있어야 함
: PR diazepam : 0.5 mg/kg (max: 20mg)
: IM midazolam : 0.2 mg/kg (max : 10mg)
: IM lorazepam : 0,1 mg/kg (max: 4mg)

(2) 마스크로 산소투여
(3) SPO2, EKG 감시 : 경련하는 동안에는 중요도 떨어짐
(3) IV 확보가 중요하며 , IO, IM, IN, PR, Buccal 등 경로도 고려할 것
(4) BST : 비열성경련에서 반드시 시행
(5) Lab: 전해질, CBC, full chemistry panel, hepatic & renal study, anticonvulsant level 확인할 것 (Subtherapeutic antiepileptic drug levels)
(6) Fever 동반 시 CNS Infection 을 고려할 것
•
백신한 환아에서는 세균성 뇌수막염의 가능성 낮다는 연구가 있으므로, LP를 할지 임상적 판단 중요
cf. 9th add “however, research supports using clinical judgment when deciding to do a
lumbar puncture because the rate of bacterial meningitis is low (0.5% to 2.4%) in a fully
immunized patient”
E3. status epilepticus : An example of one approach (Fig 138-3)
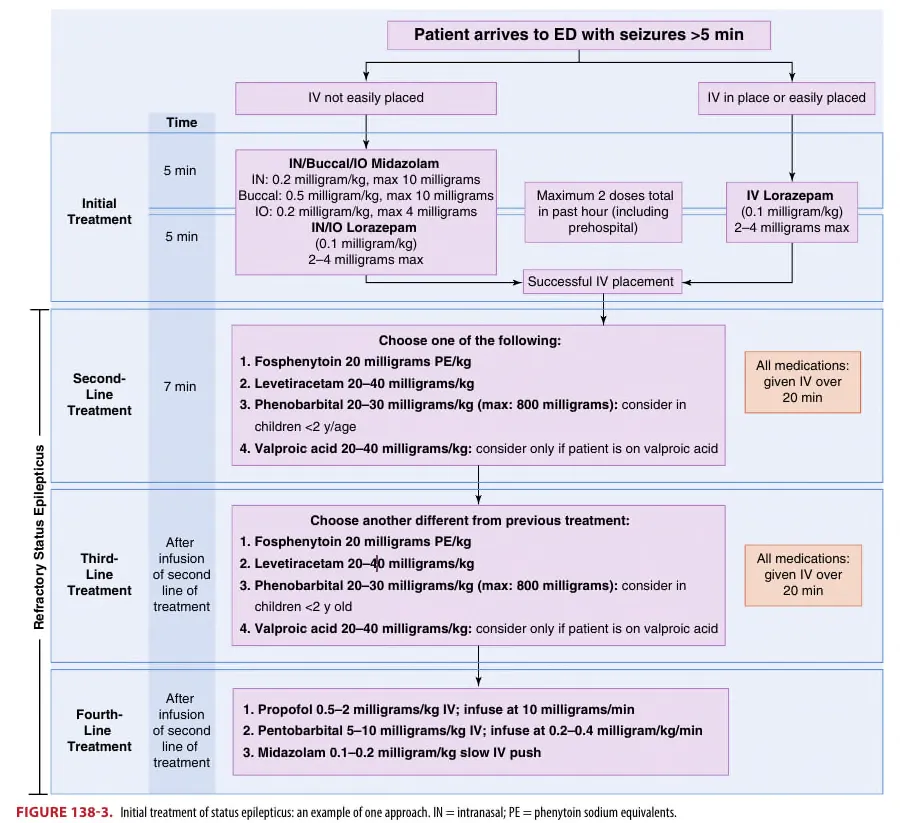
(1) First Line Treatment
•
BDZ : 1차 약제. 2회까지만 사용 (3~5 분 후)
•
2차 약제 : Fosphenytoin, Levetiracetam, Valproic acid 정도가 적당
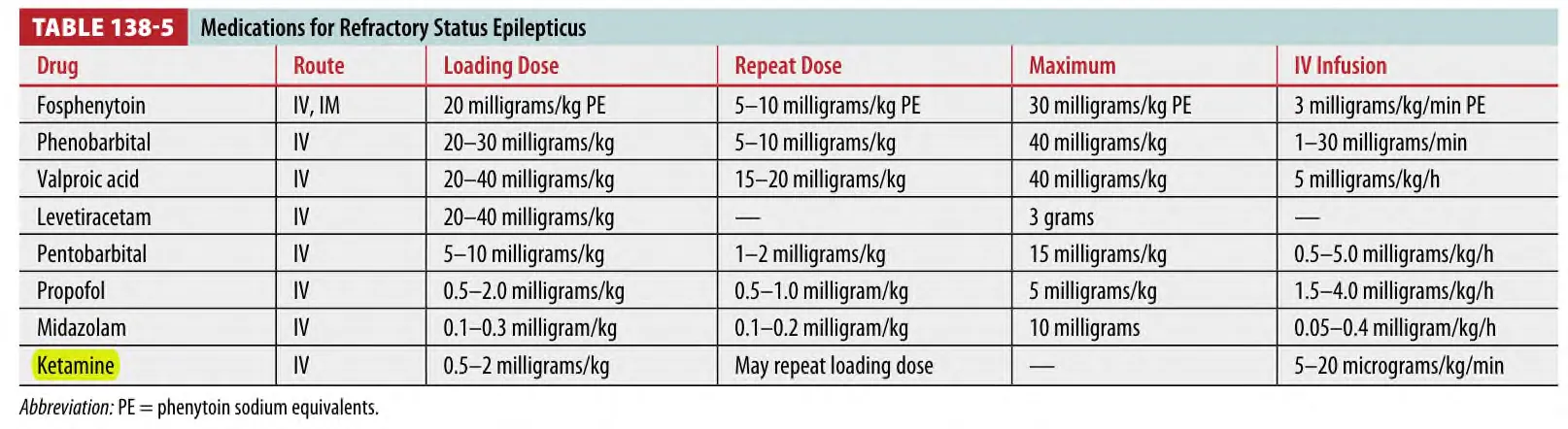
Table 138-5 summarizes the medications used for refractory status epilepticus (9th : Ketamine 추가 )
(2) Second- And Third-Line Treatments
① Phenytoin and valproic acid
: (9th 추가) Phenytoin and valproic acid, metabolized hepatically, and levetiracetam,
metabolized renally, may affect second- and third-line choices in patients with hepatic
and renal dysfunction
: Fosphenytoin (prodrug of phenytoin) : 20 PE/kg
•
Stabilizing sodium channels, neuronal calcium uptake↓
•
Phenytoin 보다 cardiac effect 가 적고 빠르게 적용 가능함
② Phenobarbital : 20~30 mg/kg (max: 800 mg)
•
2세 이하에서 고려
•
BDZ 이후 첫 번째 약제로는 잘 고려하지 않음,
: Not preferred as a second-line treatment, except in neonates
: 이유- BDZ과 same mechanism(action and bind γ-aminobutyric acid receptors) 이라서 호흡부전에 위험↑
: Most commonly used in neonates who are often maintained on daily phenobarbital for
subsequent seizure control
: Side effect - sedation and cardiorespiratory depression
③ Levetiracetam : 20~40 mg/kg
: Eliminated solely via renal excretion → no drug and food interactions
: Commonly used for maintenance therapy for multiple seizure
(than fosphenytoin (phenytoin) & phenobarbital)
④ Valproic acid : 20~40 mg
•
Valproate 투여 중인 환자에서만 고려
•
2세 미만은 간독성으로 금기 (Nelson)
: Effective for partial and generalized seizures
: Consider valproic acid for treatment of children already taking this medication who are
suspected of having subtherapeutic levels
: Hepatic failure or thrombocytopenia 유발하므로 metabolic disease 환아에서는 사용주의
(3) Fourth-Line Treatment
① Propofol
: γ-aminobutyric acid receptors differently from benzodiazepines or barbiturates and
has been shown to effectively treat refractory status epilepticus better than pentobarbital
: Action 이 빠른 대신 대사도 빨라서 Continuous infusion 적용이 필요
: Side effect - Bradycardia, Apnea, Hypotension 등 있을 수 있어서slowly infusion
: “Propofol infusion syndrome” - 24시간 이상 사용 시 주의
(Metabolic acidosis, Rhabdomyolysis, Renal failure, and Cardiac failure)
② Ketamine (9th 추가 )
: A noncompetitive N-methyl-d-aspartate – type glutamate receptor antagonist
: Refractory status epilepticus의 late stage 에 효과적
: Intubation시에도 사용하며 , ICP 올린다는 증거는 없음
③ Pentobarbital coma or continuous infusion
: Used for refractory status epilepticus not responsive to multiple anticonvulsant treatments
④ Midazolam
: Adverse effect rate 는 낮으나 , propofol & pentobarbital 보다는 Sz. recurrence가 higher rate
(4) Treatment of Glucose and Electrolyte Abnormalities
•
(9th 추가) a glucose should be checked at a minimum.
① Hypoglycemia
: Defined as at least one blood glucose concentration <47 milligrams/dL (Chap 146.참고 )
: Bedside testing is essential in seizing patients
: Treatments
Hypoglycemia with a rapid infusion of 2mL/kg of 25% dextrose in water
or 4 to 5 mL/kg [9th]( 5mL/kg [8th]) ← of 10% dextrose in water
② Hyponatremia
: Serum sodium <135 mEq/L
: Most commonly seen in infants <6 months of age and sometimes in athletes and
can cause seizures, especially if the serum sodium is <120 mEq/L.
: The goal of therapy is to correct the level to >120 mEq/L quickly & then correct
to normal levels over the next 24 hours
: Treatments
•
The seizing patient with hyponatremia with 3% NaCl 1~2 mL/kg over 20 minutes [9th]
( 3% NaCl 4~6 mL/kg over 20 minutes [8th])
or begin an infusion of 20 mL/kg of 0.9% NaCl if 3% NaCl is not immediately available
③ Hypocalcemia
: More common in neonates and young infants and may be associated with congenital
anomalies such as DiGeorge’s syndrome
: Treatments .
•
Calcium gluconate, 100mg/kg (rate<100mg/min) [9th]( ←0.3mL/kg over 5~10 min [8th])
is preferred over calcium chloride when infusing through a small peripheral IV because
calcium chloride can cause local irritation.
④ Hypomagnesemia
: Serum magnesium <1.5 mEq/L
: Treatments. - 50 milligrams/kg IV infused over 30 minutes[9th] ( 20min [8th])
