


(1) Treatments
① Unstable
VT without pulse : Defibrillation, chest compression
VT with pulse : Sedation-assisted synchronized cardioversion
② Stable
Pharmacologic agent(procainamide, amiodarone, lidocaine, magnesium)
약물에 반응 없으면 sedation-assisted synchronized cardioversion
F2. Undifferentiated wide-complex tachycardia
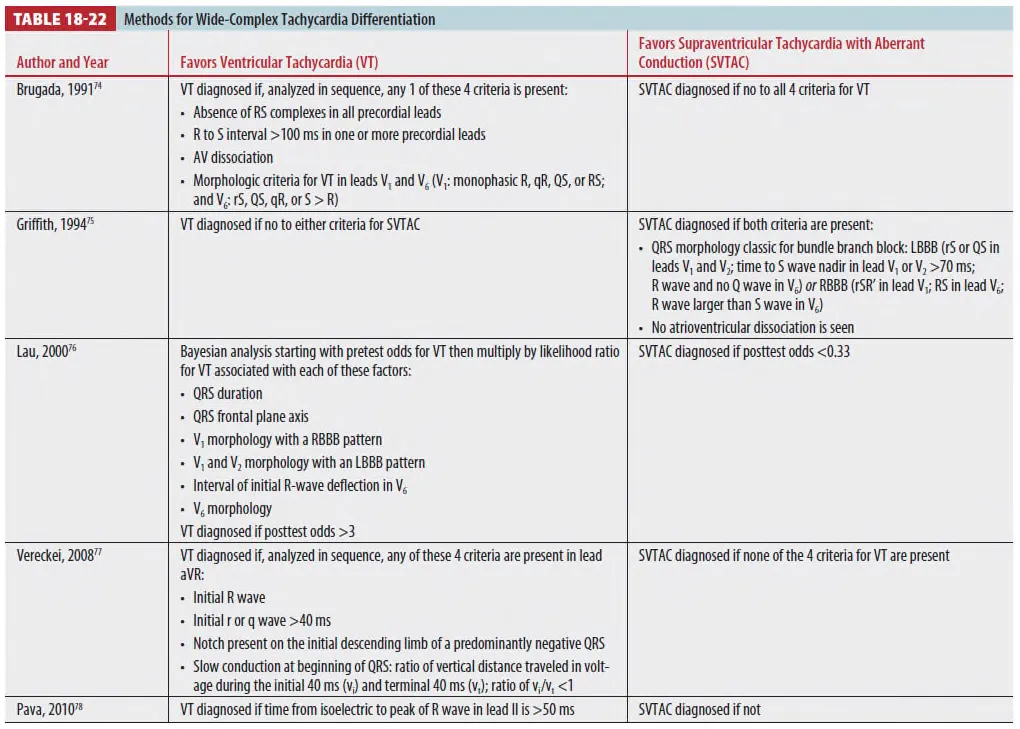
어느 것이 더 우월하다고 증명된 것은 없음 * . 단순성을 따졌을 시 Vereckei나 Pava가 선호됨.
(1) Treatments
① 구분이 어려우면 ventricular origin으로 간주하고 치료 (9판에서 삭제)
② 치료 전 hyperkalemia나 Na channel block 문제인지 등을 고려.
③ 빠른 치료가 필요할 경우 amiodarone을 사용한다. (9판에서 삭제)
④ Adenosine에 의한 반응으로 VT과 SVT with abberancy를 구분하는 데 도움이 되나,
adenosine에 반응이 있는 VT도 있어 잠재적으로 진단을 놓칠 수가 있다.
⑤ Stable한 환자는 urgent한 치료가 필요하지 않고, 진단이 불분명할 경우,
⑥ Cardiologist consult가 필요하다고 함.
F4. Ventricular fibrillation
(1) Treatments
: Chest compression & Defibrillation
Regular Wide Tachycardia 의 대처 (핵심)
Structural heart disease (US)
•
MI (ischemic VT), dilated CMP, ARVD, Cardiac sarcoidosis, HCM, VHD
•
Amiodarone
No structural heart disease
•
Adenosine으로 반응을 살펴보고 SVT 감별 -> verapamil
•
ST라면 추가적인 치료가 필요 없을 가능성이 있다
•
Preexcitation인 경우 heparin을 주고 DC cardioversion이 원칙, AP찾아보자
혈압이 떨어지면 sync DC cardioversion
VT는 AV dissociation, conduction delay를 살펴본다.
•
P wave 찾기, VA conduction 찾기, QRS 초기 전도속도 확인
Treatment
Sinus tachycardia (ST) c abberrancy (BBB)
•
Symptomatic chronic ST --> beta blocker(metoprolol), Ivabradine
SVT c aberrancy (BBB)
•
Adenosine 6mg --> 12 mg --> verapamil 5mg --> 10mg (->digoxin -> B-blocker)
•
Recur인지 fail인지 감별할 것!
: sinus thythm이 잠깐이라도 나타난 경우 용량증가, fail인 경우는 약 변경
VT
•
Unstable -> DC cardioversion
•
Stable -> structural heart disease (procainamide > amiodarone -> Lidocaine)
-> idiopathic (adenosine, verapamil, metoprolol, ablation)
A-flutter c aberrancy (BBB)
•
Rate control (diltiazem, verapamil, esmolol)
Antidromic AVRT or A-flutter c WPW
•
Procainamide, ibutilide
•
DC cardioversion (heparin 5000U)
•
AV nodal drugs 금기 (B)
Cf) A-fib c WPW (irregular)
•
Procainamide and ibutilide
•
Amiodarone(x), DC cardioversion
F5. Torsade de Pointes
(1) What is Torsades de Pointes?
•
Polymorphic VT in patients with QT prolongation
•
Peaks of the QRS “TWIST” - Twisting of the points –
•
Usually terminates spontaneously
•
Can degenerate to VF

TdP은 QT prolongation을 가진 환자에서 나타나는 특정 모양의 polymorphic VT입니다. 불어로 twisting of the points라는 뜻을 가진 것처럼 꼭지점이 나선형을 이루 듯 보이는게 특징이며, 대부분 짧은 시간내에 회복되나, 간혹 v. fib.으로 진행되고 sudden cardiac arrest 혹은 death를 유발할 수 있기에 주의를 요합니다.
Long QT syndrome
•
Congenital vs Acquired
•
Over 17 different gene variants
•
QT-prolonging disease or meds (www.crediblemeds.org)

TdP의 전제 조건이 QT prolongation이기 때문에, 이를 이해하기 위해서는 Long QT synd.을 알아야합니다. LQTS 은 크게 congenital과 acquired로 나눌 수 있는데, congenital은 지금까지 밝혀진 유전자 변이가 17개가 넘습니다. 그 중 LQTS 1, 2, 3이 전체의 약 80프로 이상을 차지합니다. Acquired의 경우 QT prolongation을 유발하는 약물 혹은 질환에 의해 발생하고, 종류가 매우 다양합니다. 이 사이트에 가입하시면 편리하게 검색할 수 있으니 참고 하시면 되겠습니다.

Concomitant risk factors

Therapeutic Advances in Drug Safety. 2012 Oct.; 3(5)
Congenital LQTS - Pathophysiology
•
Cardiac channelopathy
•
Sympathetic innervation imbalance
LQTS 의 치료는 type에 따라 차이가 있습니다.
Congenital LQTS은 심장의 ion channel 의 교란와 교감신경 innervation의 불균형에 의한 것이라는 가설이 지배적입니다. Action potentia을 나타내는 왼쪽 그림의 보라색은 depolarizing, 주황색은 repolarizing channel 입니다. LQT1 은 slow potassium channel, 2는 rapid channel, 3는 sodium channel의 문제가 있습니다.
재분극 문제의 경우 정상상태에서는 칼륨이 세포 밖으로 나가면서 세포 안을 다시 음의 전위로 돌려놓아야하는데 이게 느려지면 3단계가 길어지고 양의 상태로 오래 머물어서 QT가 길어집니다.
탈분극의 과다는 원래 닫혀야 하는 채널이 계속 열려 있으면서 양이온이 계속 세포내로 유입되어 세포 안이 음이온으로 돌아가는 시간이 밀립니다.
흥미로운 사실은 여기서 rapid potassium channel이 바로 drug induced LQTS의 원인이라는 것입니다.

Circ Arrhythm Electrophysiol 2016; 9:1
Acquired LQTS - Pathophysiology
•
Mostly due to drugs
•
Blocking IKr current

Journal of the American College of Cardiology, Volume 72, Issue 14, 2018
즉, LQT2와 drug induced LQTS의 병태생리가 유사하다는 것입니다.
앞에서 보던 약들이 있죠.
Triggers of arrhythmia in LQTS
•
Congenital = Adrenergic surge
•
Acquired = Pause dependent

Circ Arrhythm Electrophysiol. 2012 Dec;5(6):e119-20.
대부분 congenital은 운동하다가 생기는 adrenergic surge 로 인해 부정맥이 유발되고, acquired는 brady 혹은 pause dependent이다. 라고 하는데, 이는 반만 맞는 얘기입니다. 이 표는 genotype에 따라 cardiac event가 나타나는 비율인데, 보시다시피 LQT1 은 운동에 의해 75%가 발생하고 LQT2는 emotion 변화나 휴식 때, 3는 휴식 때 많이 발생합니다.
Treatment of TdP

Uptodate에 있는 TdP의 치료입니다. Isoproterenol은 acquired LQTS에만 있습니다. 시간 관계 상 다른 치료는 생략하겠습니다.
2017 AHA/ACC/HRS Guidelines

2017년 가이드라인에서도 isoproterenol은 acquired QT prolongation이 있는 반복적인 TdP 환자가 IV Mg.에 호전이 없을 때 쓸 수 있다고 되어 있습니다.
2022 ESC Guidelines
•
Hypomagnesaemia and/or hypokalaemia may be associated with Torsades de pointes (TdP)
•
Intravenous magnesium is an effective therapy for TdP even in the absence of hypomagnesaemia
•
In refractory cases of recurrent TdP in the setting of acquired long QT, the arrhythmia can be suppressed by increasing the underlying heart rate using isoproterenol (isoprenaline) or transvenous pacing.
22년 ESC 가이드라인 역시 acquired 에서 발생하는 recurrent TdP 환자에서 isoproterenol 혹은 transvenous pacing을 시도해볼 수 있다고 되어 있습니다.
2022 ESC Guidelines
•
LQT1 : 운동 유발
LQT2 : 감정 스트레스
LQT3 : 수면 or 휴식 시 유발
•
All LQTS patients should avoid
Hypokalemia
QT-prolonging medications
Genotype-specific triggers
•
Beta-blockers are also recommended in all LQTS patients à Acquired???



2022 ESC Guidelines

2006 ACC/AHA/ESC Guidelines

2006년도 마찬가지로 recurrent pause-dependent TdP 환자 중 congenital이 아닌 사람에서 시도해볼 수 있다고 되어 있습니다.
Pause dependence?
When TdP is initiated by “Short-Long-Short” sequence

European Heart Journal, Volume 25, Issue 23, December 2004
pause-dependent 라는 말이 나오는데, 이건 TdP이 short-long-short sequence에 의해 유발되는 것을 의미합니다. C1이 C2, 0 보다 긴 것이 특징이고, PVC가 나타나면서 pause가 생겨 long-short sequence를 만들어 다음 ectopic beat가 R on T 를 유발하는 것입니다. 이런 현상 역시 LQT2에서는 흔하지만, 1에서는 거의 없다고 합니다.


LQT1 broad T wave
LQT2 low-amplitude T wave
LQT3 peaked T wave
1.
Acquired LQTS의 주요 형태적 특징
후천성에서는 T-wave 자체의 모양보다 QT 연장의 진행 양상과 U-wave의 출현이 더 중요합니다.
T-U Fusion (가장 전형적): 뚜렷한 U-wave가 나타나면서 앞선 T-wave와 합쳐져 거대한 파형을 만듭니다. 이로 인해 실제 QT보다 훨씬 길어 보이는 'QU 간격'이 형성되며, 이것이 TdP의 직전 단계인 경우가 많습니다.
Low Amplitude, Broad T-wave: 약물(특히 $I_{Kr}$ 차단제)에 의한 경우 T-wave의 진폭이 낮아지면서 옆으로 넓게 퍼지는 양상을 보입니다.
T-wave Alternans (T-파 교대): 비트마다 T-wave의 모양이나 극성(Polarity)이 바뀌는 현상으로, 심실 재분극의 극심한 불안정성을 의미하며 TdP 발생의 강력한 전조 증상입니다.
Isoproterenol can be given to…
•
Recurrent pause-dependent TdP, who do not respond to Mg
1. Acquired LQTS
2. Not congenital
•
Should NOT be given to pt. with angina
•
만능 X
정리해보면 isoproterenol은 Mg에 반응하지 않는 acquired LQTS에 의해 발생한 recurrent pause-dependent TdP에서는 확실히 쓸 수 있습니다. 그렇다면, congenital은 안될까요? 참고할만한 experimental study입니다. LQT3은 isoproterenol을 투여한 경우 TdP의 발생 빈도가 줄었고, LQT2는 초기 투여에는 발생빈도가 증가하다가 10분 동안 유지하였더니 빈도가 감소하였습니다. LQT1은 투여 전까지는 발생율이 0%였는데 isoproterenol을 투여하니 TdP이 유발되는 것을 볼 수 있습니다.
Treatment of polymorphic VT (2025 AHA)
•
QT interval과 상관없이, all PMVT 는 hemodynamically & electrically unstable !
•
Monomorphic은 cardioversion이 VF risk를 감소
•
PMVT 는 CANNOT BE synchronized reliably
⇒ Requires high energy unsynchronized shock !
•
Defibrillation으로 TdP 를 termination 시키는 것은 재발을 방지하진 않음

