


A. Introduction and epidemiology
A1. AKI 정의
: Toxic wastes 축적과 internal homeostasis 소실로 인해 수시간~수일에 걸쳐 신 기능이 악화되는 것
(신기능에 기반한 정의는 아래 Table 88-1 참조)

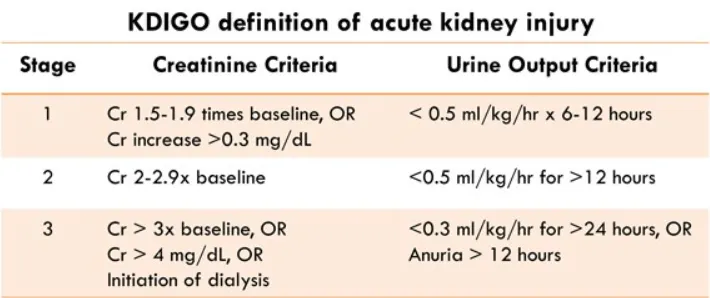
(1) KDIGO definition
: 아래 세 가지 기준 중 하나라도 만족 시, 급성 신손상으로 정의한다
•
48시간 이내 serum Cr이 0.3 mg/dL 이상 상승
•
7일 이내에 serum Cr의 baseline이 1.5배 이상 상승
•
6시간 이상 지속되는 UO < 0.5 ml/kg/hr
A2. Community-acquired AKI
: Volume depletion, medication, infection, urinary obstruction의 원인으로 가역적인 매커니즘 상태,
A3. Hospital-acquired AKI
: 병원 내에서 생기거나 나빠지는 경우로 사망률은 27~62%
AKI의 양쪽 type의 사망률은 AKI의 연령과 심각도와 연관관계가 있다.
B. Pathophysiology
•
Normal GFR : 120mL/min/1.73m2 → 10년마다 8정도씩 감소
•
대부분의 Intrinsic AKI 의 원인은 ischemic injury or ischemic tubular necrosis이고 신실질이
영향을 받을만큼 신관류가 감소할 때 발생한다.
•
남아있는 Nephron pool의 크기에 따라 GFR이 비례하여 회복된다.
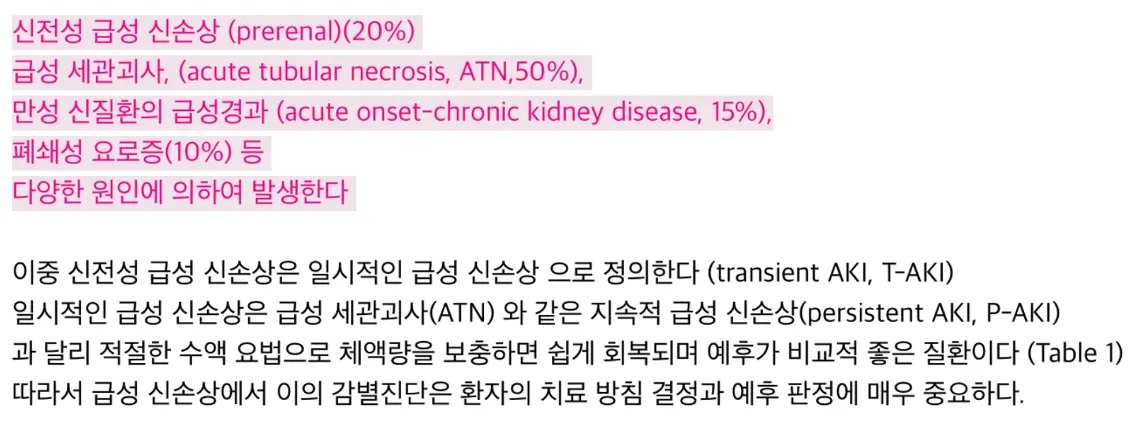
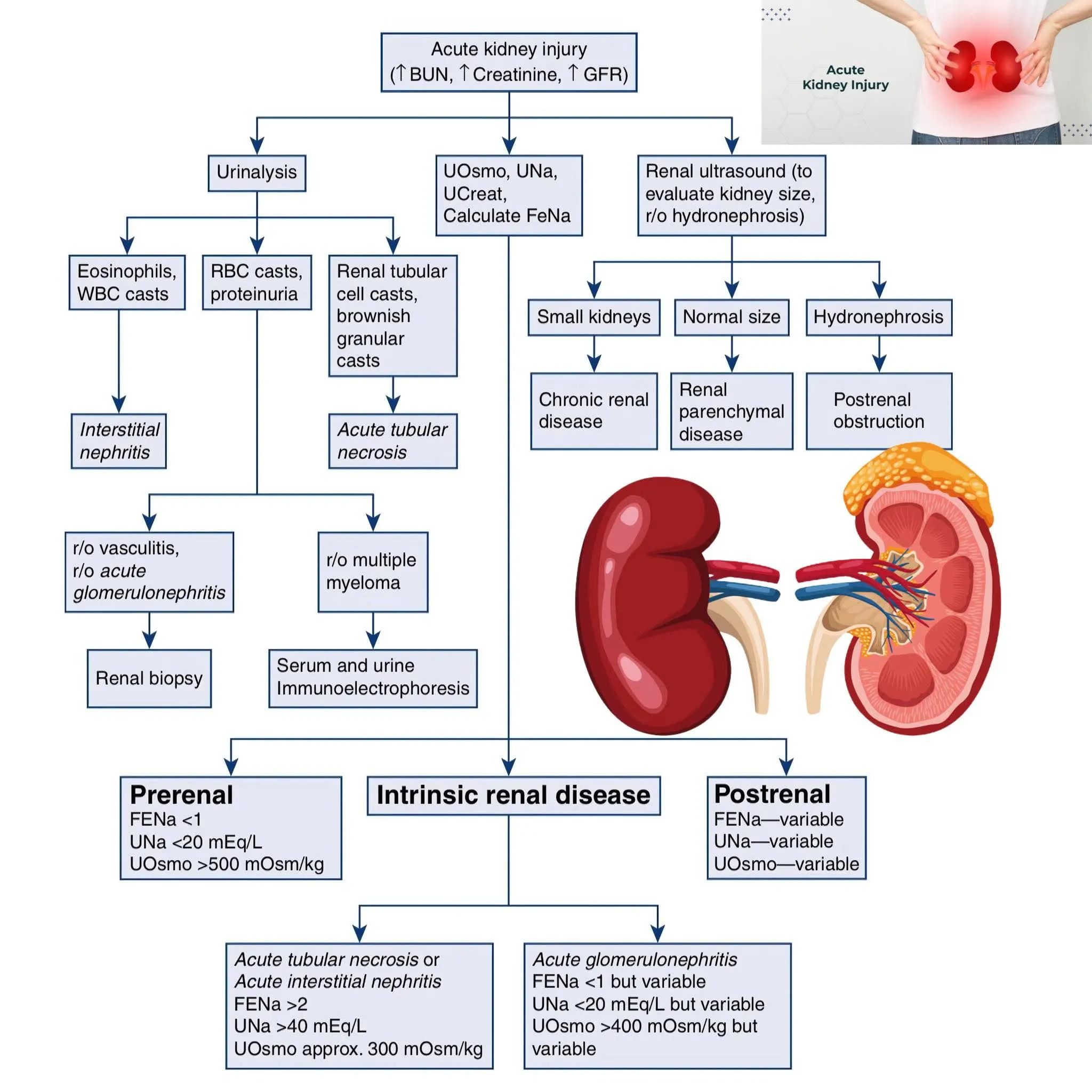
B1. Classification
(1) Prerenal (decreased perfusion of a normal kidney)
(2) Intrinsic (pathologic change within the kidney itself)
(3) Postrenal (called postobstructive, obstruction to urine outflow)
→ AKI 대부분의 원인에서 전체적 혹은 부분적으로 신혈류의 감소가 final common pathway
C. Clinical features
C1. History and comorbidities
(1) AKI는 요독증이 심하게 진행될 때까지 그 자체로 거의 증상을 나타내지 않는다.
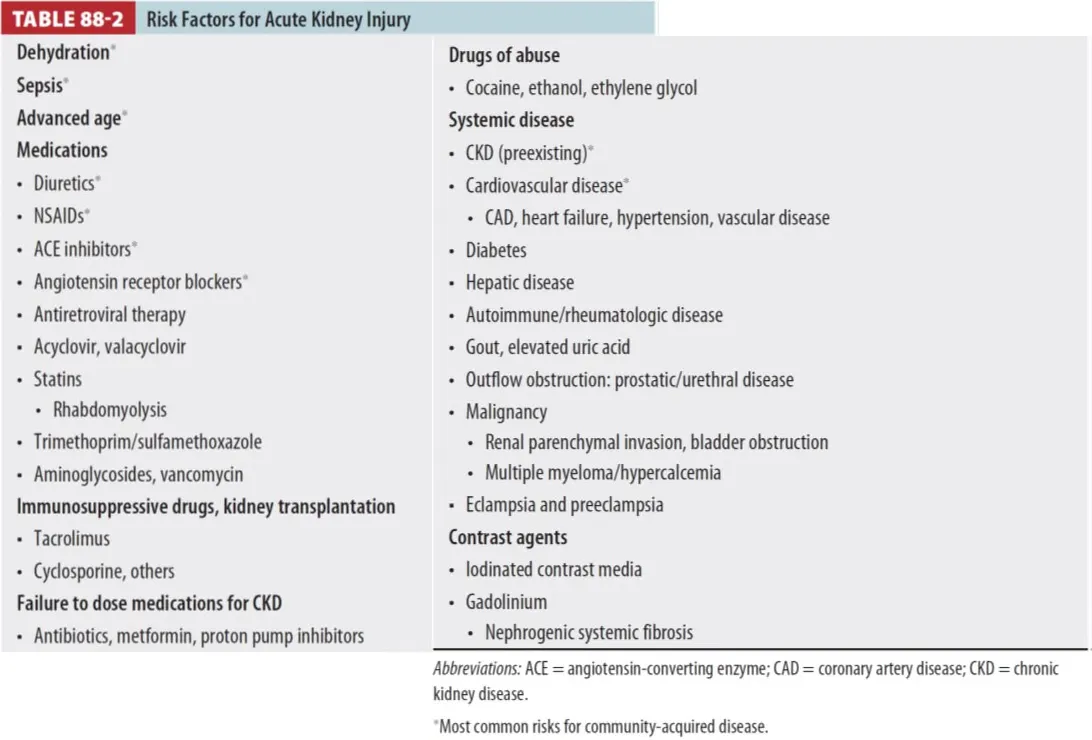
(2) 증상 (nausea, vomiting, drowsiness, fatigue, confusion, if untreated, coma)이 AKI의 기저
원인 (Table 88-2 참조) 과 연관되어 나타나는 경우가 많으므로 이에 따라 즉시 신기능을 평가한다.
C2. Prerenal AKI
(1) Sx. : Thirst, orthostatic light-headedness, decreased urine output
(2) Excessive vomiting, diarrhea, urination, hemorrhage, fever, sweating
(3) Endothelial leak & third space loss : sepsis, pancreatitis, burns, hepatic failure
(4) Heart failure 및 이뇨과다 (Overdiuresis)
(5) 수분섭취 감소에 의한 Hypovolemia
C3. Intrinsic renal disease
(precipitating cause의 Sx.으로부터 예상 가능한 경우들)
(1) 심정지, 중증패혈증, 기타 전신 저혈압 → Ischemic AKI
(2) Flank pain, hematuria → Crystal-induced nephropathy, nephrolithiasis, papillary necrosis
(3) Rhabdomyolysis, 최근 수혈 후 Hemolysis → Pigment-induced AKI
(4) Dark urine, edema /with or w/o sx. (fever, malaise, rash), 선행하는 인두염 또는 피부감염
→ Acute glomerulonephritis
(5) Fever, arthralgia, rash → Acute interstitial nephritis
(6) Severe flank pain → Acute renal arterial occlusion
(7) Cough, dyspnea, hemoptysis → Goodpasture's syndrome, Wegener's granulomatosis
C4. Postrenal AKI
(1) 전립선질환, 고령, 도뇨관 유지중
(2) 핍뇨와 다뇨의 반복 → Obstruction
D. Physical examination
D1. 비정상적 volume status 평가가 중요
Dehydration 정도를 알기 위해 점막, 경정맥, 폐 청진, 말초 부종, tissue turgor 등을 진찰
D2. Fluid overload 의심
(1) 급속한 체중증가
(2) 말초 및 facial edema
(3) 폐하부 청진에서 pulmonary rales or dullness
E. Diagnosis
1.
Type 감별 : Prerenal, postrenal, intrinsic → ED에서 치료방침 결정에 중요.
2.
Hypovolemia : Base deficit, lactate↑, CVP ↓, US에서 inferior vena cava의 collapse
3.
ECG : 가장 빠른 screening test for hyperkalemia (but sensitivity 낮음 : 14%~60%)
4.
Chest x-ray : Increased volume, effusion or pneumonia
5.
Large postvoid bladder residual volume (>125mL)→ Bladder outlet obstruction
6.
Anuria (<100ml/day)는 prerenal, postrenal, intrinsic에서 다 나타날 수 있음.

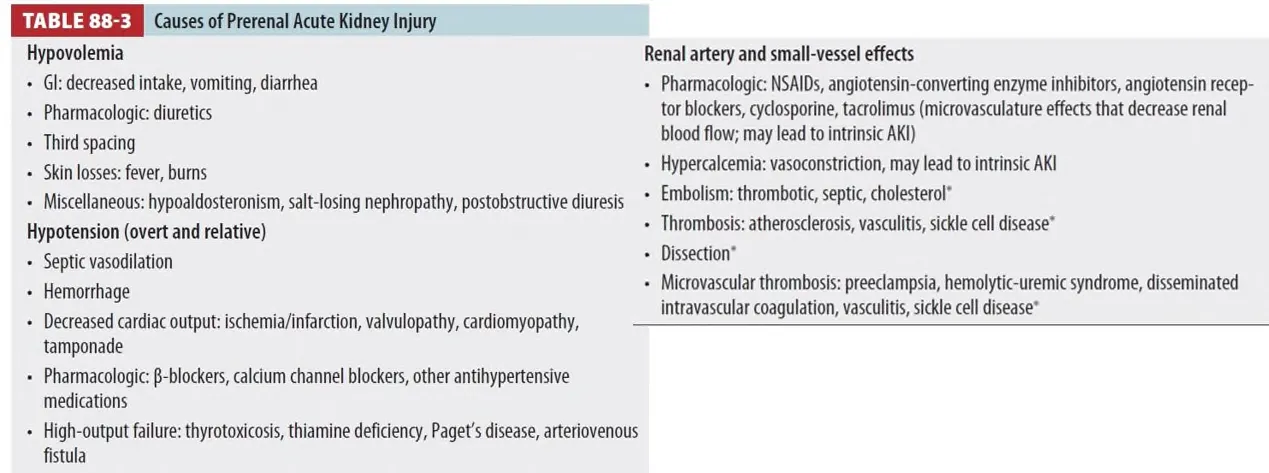
F. Prerenal acute kidney injury
F1. Cause of prerenal azotemia
(1) Volume loss
(2) Hypotension
(3) Large & small renal artery의 disease
1.
Ischemic and nephrotoxic 상태 후 intrinsic AKI로 진행 가능
G. Postrenal acute kidney injury
1.
고령에서 22%정도의 비율
2.
Prostatic hypertrophy가 가장 흔한 원인
3.
양쪽 성별의 고령 환자에게서 고려
(1) Indwelling urinary catheters
(2) GU surgery
(3) Known or suspected abdominal malignancy
(4) Nephrolithiasis
(5) Retroperitoneal disease
(6) Urinary sphincter에 영향을 주는 medication
H. Intrinsic acute kidney injury
•
Community에서는 드물지만 병원 내에서는 가장 흔함
•
Community : Drugs, infection, vascular event / Hospital-aquired : Toxic & ischemic insults

H1. Contrast-induced nephropathy
(1) 응급실에서의 IV contrast 사용으로 Radiocontrast-induced nephropathy 발생 가능
•
주입 후 48~72 시간 내에 Cr level baseline의 25% 이상 증가했거나
•
절대량으로 0.5 mg/dL (44 μmol/L)의 상승을 보일 때
(2) 이미 CKD가 있는 환자에게서 촬영 전 hydration을 통해 신기능악화를 예방할 수 있다.
H2. Crystal-induced nephropathy
(1) Renal tubule 내 crystal 침적이 tubular epithelium에 mechanical, inflammatory injury 일으킴.
(2) Urinary pH가 crystal의 생성에 영향을 줌.
(3) Tumor lysis syndrome (Serum uric acid↑), medication (acyclovir, sulfonamides, indinavir,
triamterene)으로 인한 uric acid의 상승이 흔한 원인
H3. Angiotensin-converting enzyme inhibitors
(1) ACE inhibitor의 사용으로 Cr이 보통 10~20% 상승시키나, 드물게 급격한 상승을 일으킴
(2) ACE inhibitor 사용 시작 후 AKI 발생 시 bilateral renal artery stenosis를 고려해야 한다.
(3) Mild hyperkalemia도 자주 동반됨.
H4. NSAIDs
(1) GFR과 renal blood flow 양쪽을 감소시키기 때문에 AKI의 원인이 될 수 있다 (prerenal)
(2) 지속적인 사용은 interstitial nephritis (intrinsic AKI)의 원인 될 수 있다.
(3) Risk factor
① Older age
② Chronic renal insufficiency
③ Congestive heart failure
④ Volume depletion
⑤ 이뇨제 또는 ACEi 의 동시사용
H5. Antibiotics
(1) 항생제 (특히 aminoglycosides)가 iatrogenic renal injury의 중요한 원인이 된다.
(2) Vancomycin, ceftriaxone, sulfamethoxazole/trimethoprim, amoxicillin, cefazolin,
fluoroquinolones 가 AKI를 자주 일으킨다.
(3) Antiretroviral, acyclovir, valacyclovir가 항바이러스제에 의한 AKI의 주요 원인이 된다.
H6. Pigment nephropathy
(1) Hemoglobin(hemolysis), Myoglobin(rhabdomyolysis)이 renal tubule에 침적
H7. Glomerulonephritis
(1) AKI의 uncommon cause
(2) Edema, proteinuria, hypoalbuminemia, hyperlipidemia : nephrotic syndrome
(3) Hematuria, red blood cell cast, urine output 감소, HTN : nephritis syndrome
(4) Postinfectious, toxic exposure, immune disorder (SLE)와 연관
I. Diagnostic testing
I1. Creatinine and GFR
(1) Renal function이 없는 환자의 경우 (GFR=0), serum Cr level은 하루에 1~3 mg/dL가량 상승한다.
•
천천히 상승하는 경우는 잔존 신기능이 있음을 시사하고,
•
더 빨리 상승하는 경우 rhabdomyolysis 시사
(2) Serum Cr의 상승은 function의 저하가 시작된 후 48시간가량 지난 후 일어난다.
(3) Cr clearance는 완벽하지는 않지만 GFR을 측정하는데 사용되고 이는 ED에서 유용
(4) 근육량이 적은 사람(고령, 여성)의 경우 Cr 결과보다 실제 GFR이 낮게 나온다.
(5) Glomrulonephritis는 Cr의 tubular 분비를 증가시키고, trimethoprim, cimetidine, salicylates 등은
Cr의 tubular 분비를 감소시킴
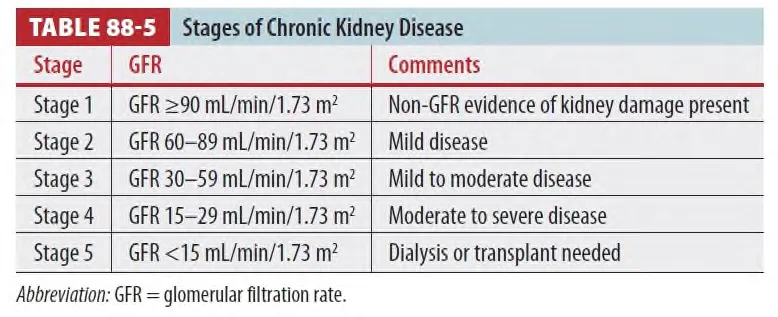
(6) Normal kidney function is a GFR >90 mL/min/1.73m2
2. Cystatin C
(1) Cystatin C 단백질은 Cr와는 다르게 infections, inflammatory, neoplastic condition에 영향을 받지
않고 일정하게 생성되며, 식이, 약물, 몸무게의 영향을 받지 않는다.
(2) Cr와 같이 AKI가 생긴 뒤 24~48 시간 뒤 측정된다.
(3) 사망, 만성신부전의 진행, 투석여부를 더 정확하게 예측할 수 있다.
3. Urine output
(1) 소변 배출량을 정확하게 측정하려면 RIFLE (Risk, Injury, Failure, Loss, End-stage) 기준에서
요구하는 AKI를 충족하기 위해 6시간 이상 소변 카테터를 유지하여야 함
4. BUN to Creatinine ratio
(1) Volume status 평가에 이용
(2) Urea는 tubule에서 sodium과 함께 재흡수 (Cr는 재흡수가 안됨 )
→ Volume이 부족하여 sodium 재흡수가 많이 일어날 경우, urea clearance가 GFR의 30% 가량으로
낮아지고, volume이 충분할 경우 urea clearance가 GFR의 70~100% 가량으로 상승한다.
(3) Prerenal failure의 경우, urea 재흡수가 많아지므로, BUN/Cr ratio가 10 이상이 된다.
(4) BUN의 감소 : Malnutrition, Hepatic synthetic dysfunction
(5) BUN의 증가 : Protein loading, GI hemorrhage, Trauma
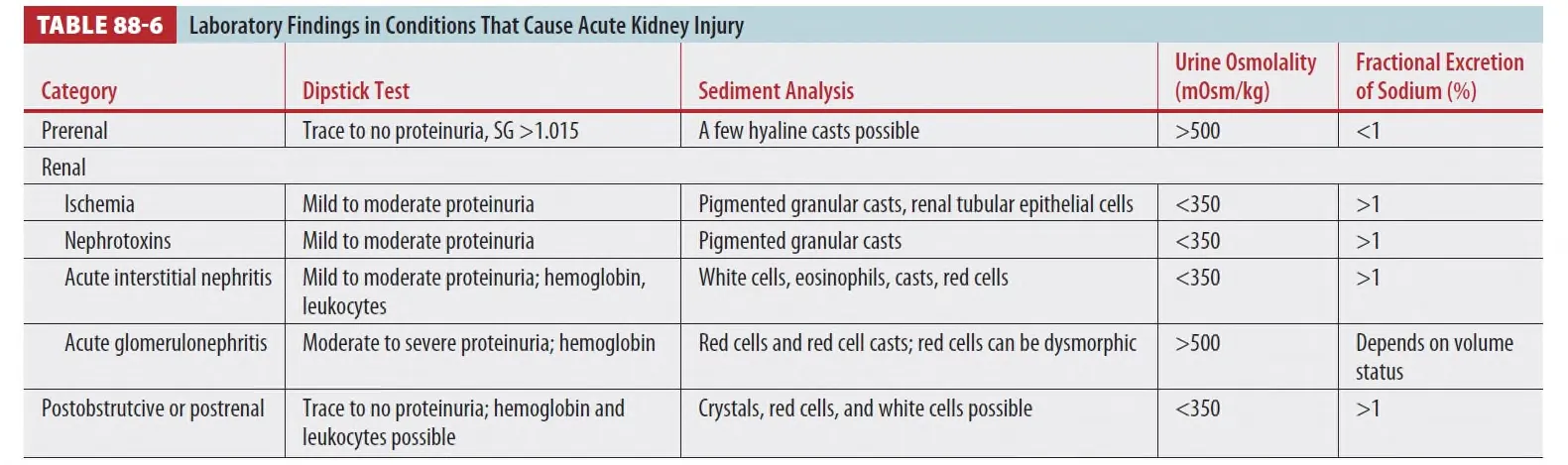
5. Fractional Excretion of Sodium
(1) FeNa = UNa/PNa ÷ UCr/PCr, where U = urine and P = plasma
(2) FeNa<1 이면 hypovolemia = Prerenal
: 예외로 Glomerulonephropathy (Intrinsic AKI)는 FeNa가 1 미만으로 나올 수 있다.
Tubular concentrating capacity↓ → Na 배출↓로 FeNa가 <1 일수도 있음
(3) 대개 ATN과 같이 tubular injury가 있는 경우에는 volume이 부족하여도 FeNa가 1%보다 큰 수치가 나올 수 있다. (농축기능의 손상 후 묽은 소변이 나옴)
6.Urinalysis
(1) Microscopic hematuria, Cast, Dysmorphic cells : Gromerulonephritis
(2) Proteniuria, tubular epithelial cell : ATN
(3) Hyaline cast : prerenal AKI 이거나 정상
(4) Pigmented granular cast : Ischemic or toxic tubular injury
(5) Brown granular casts : hemoglobinurea나 myoglobinurea 가 있을때 흔함
(6) Myoglobinuria : dipstik에서는 RBC (+) 인데 Microscopic에서는 RBC (-)
(7) Crystal은 정상소견에서 나타날 수 있다.
7. Imaging
(1) Renal US : test of choice
(2) Hydronephrosis → Obstruction을 시사
(3) Kidney dimension < 9 cm → Chronic kidney disease를 시사
(4) Intermittent 하거나 partial obstruction의 경우, hydronephrosis가 없을 수도 있으며,
retroperitoneal fibrosis에서는 complete obstruction이 있더라도 hydronephrosis가 없을 수 있다.
(5) Noncontrast CT : Hydronephrosis에 대해 US와 동등한 sensitivity, Obstruction site와 cause를
파악하는데 장점.
(6) Functional obstruction 의심되는 경우 이뇨제 투여 전후의 radionuclide scans와 MR urographs
검사를 시행함.
J. Treatment
•
Hypovolemia를 교정
•
Sepsis, MI, respiratory failure, acute decompensated heart failure, electrolyte disturbances,
acidosis, volume overload, urinary obstruction 확인하여 치료.
J1. Volume replacement
(1) crystalloid를 이용하여 교정.
•
balanced crystalloid가 normal saline 보다 약간의 이득이 있다.
(2) 투여 속도와 용량
•
저혈압(수축기 혈압 <100mmHg 또는 기준치 대비 20mmHg 이상 감소) 및 저혈량 상태:
◦
250~500mL crystalloid를 30분 이내에 볼루스(rapid bolus)로 투여
◦
혈압과 소변량, 폐부종 등 합병증 여부를 관찰하며 반복 투여 가능
◦
목표: 혈압 회복(수축기 혈압 >100mmHg), 소변량 증가가 첫 반응
•
정상혈압이나 경계선 저혈압:
◦
투여 속도와 용량은 임상적으로 판단하여 조절
◦
과도한 수액 투여는 피하고, 필요시 소량씩 반복 투여하며 환자 상태를 자주 재평가
•
총 투여량:
◦
초기 resuscitation에서는 일반적으로 1~2L까지 투여할 수 있으나, 각 볼루스 후 임상 반응(혈압, 소변량, 폐부종 등)을 반드시 확인
◦
폐부종 등 fluid overload 징후가 나타나면 즉시 중단 및 조치.
•
정맥 수액 투여 후:
◦
환자가 volume replete(적절한 혈액량 상태)가 되면, 추가 수액은 제한(일반적으로 24시간 내 750mL 이하로 제한)
•
Volume overload를 막기 위해 침습적 혈역학적 모니터 또는 bedside US 등을 이용
(IVC가 흡기시 수축하는 것을 확인)
(3) 추가적 고려사항
•
목표 혈압: 평균동맥압(MAP) 65mmHg 이상 유지
•
반응 없을 시:
◦
반복 볼루스에도 혈압 회복이 안 되면, 바소프레서(혈관수축제) 고려
•
수액 과잉 투여 주의:
◦
과도한 수액은 폐부종, 심부전 등 합병증 위험 증가
•
소변량 증가가 가장 빠른 개선 신호
J2. Prevent renal injury
(1) AKI의 원인이 될만한 약물은 멈추어야 한다.
(2) Renal dose로 medication을 사용하고, contrast를 사용할 경우 renal function을 먼저 확인한다.
① GFR 30~59 : 조영제 사용 시 득실 확인하고 진행
② GFR <30 : Avoid IV contrast
•
Major trauma나 Aortic dissection, STEMI 같은 경우는 risk 상관없이 조영제 사용.
(3) 조영제 CT가 예정된, 비정상적 신기능 환자에서 수액 치료
•
적정 속도 및 용량은 알려지지 않았지만, 주로 lactate Ringer 용액이나 normal saline 500~1000ml을 CT 촬영 직전과 직후에 주입한다. (urgent dehydration 시에는 추가용량이 필요)
J3. Relieve urine outflow obstruction
(1) 신장 기능의 영구적인 상실은 complete obstruction 상태에서 10~14일 동안 발생한다.
(2) UTI의 합병증에 의한 obstruction은 CKD risk의 저명한 상승을 가져온다.
(3) Urethral, ureteral obstruction, sphincter dysfuction을 고려해야 함.
J4. Fluid overload 교정
•
Fluid overload는 AKI 환자의 사망률 상승과 연관이 있다.
•
AKI 환자에게서 fluid overload가 없을 경우 이뇨제 사용은 권장되지 않음.
•
Fluid overload에 대한 이뇨제의 대체치료로는 투석이며, 이뇨제 치료 반응 없으면 투석의 적응증
•
Furosemide stress test은 mild AKI 상태에서 신기능 악화를 예측할 뿐 아니라 이뇨제의 민감도를
결정하기 위해 실시한다.
•
Mannitol과 low(renal) dose-dopamine은 효과가 없다.
J5. Hypertension 교정
(1) Fenoldopam과 nicardipine이 치료에 주로 사용된다.
J6. Metabolic acidosis 교정
(1) pH가 < 7.1일 때 치료를 고려한다.
(2) Anuria or fluid overload 치료 시 투석이 선호된다.
(Sodium bicarbonate를 안전하게 사용하려면 소변 흐름과 fluid load를 견디는 능력이 필요함)
7. Electrolyte disorders 교정
(1) Hyperkalemia (PR interval prolongation, peaked T waves, QRS coplex widening) 시
치료를 고려한다.
8. Glomerulonephritis
(1) Renal biopsy, corticosteroids, cyclophosphamide, plasmapheresis 고려
(2) 신장내과 협진 시행.
9. Disposition and consultation
(1) Mild AKI (AKNI stage I)은 ED에서 경과관찰
(2) Severe AKI이거나 치료에 호전을 보이지 않을 경우 입원 고려
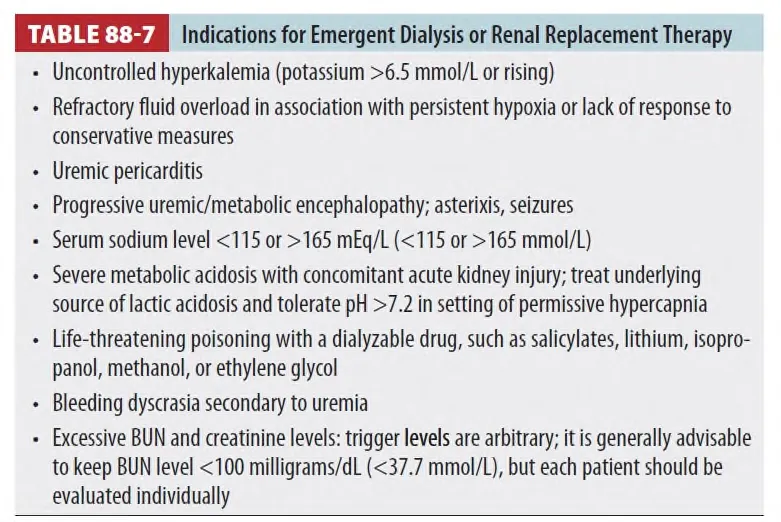
10. Dialysis/Renal replacement therapy
(1) Renal replace therapy의 시기에 대해서는 논쟁 중이다.
(2) Indication은 Table 88-7 참고
K. Special population
1. Cardiorenal syndorme
•
심장과 신장의 병태생리적인 장애로, 한 장기의 장애로 다른 장기의 급성,만성 질환을 유발
(1) Type 1 : 급성 심장기능의 악화로 AKI를 유발
(2) Type 3 : (renocardiac syndrome) AKI에 의한 acute cardiac injury
(3) Type 2 & 4 : chronic
(4) Type 5 : 2차적인 전신적인 상태 (sepsis)
(5) Serum creatine과 serum B-type natriuretic peptide를 비교 baseline과 비교 더 높은 비율로
상승한 부분으로 renal or heart disorder를 감별한다.
(6) 치료 : 심부전의 보상 + Ultrafilteration (fluid overload를 조절)
(7) 생명을 위협하는 hyperkalemia, 조절되지 않는 pulmonary edema 경우 즉각적인 ultrafilteration
이나 다른 신대체 요법을 고려한다.
2. IV contrast in patients taking Metformin
(1) 2형 당뇨병에서 자주 쓰이는 약물인 metformin에서 가능 큰 부작용은 metformin-associated lactic acidosis
(2) GFR이 30~60 사이인 환자에게서 iodinated contrast media를 사용하기 전에는 일시적으로
metformin 투약을 중지시켜야 하며, 주입 후 48시간 뒤 Cr을 확인 후 투약을 재시작해야 한다고 권고
(3) eGFR <30 환자에게서 조영제 주입 전에 metformin을 투약 중지시켜야하며, 48시간 동안 유지

