

A. Coronal section of the anorectum

B. Examination
•
Anoscopy, 필요 시 proctoscopy를 포함한 항문과 직장의 careful examination 없이
definitive diagnosis는 없다.
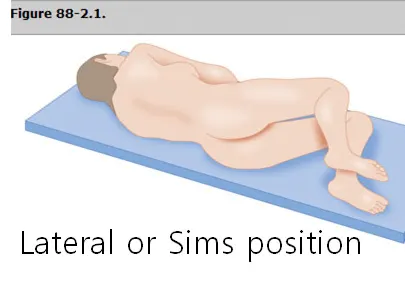
B1. The lateral or Sims position
(1) 환자를 왼쪽으로 눕게 한 상태에서 좌측 다리는 펴고 우측 다리와 고관절은 굽히는 자세로,
일반적인 직장수지검사에 적절하며, 노인, 임산부에게 선호되는 자세
(2) Upper buttock을 들어 올리면 perianal area가 더 잘 노출되고 이 자세로 anoscopy를
시행할 수 있다.
B2. Supine, lithotomy position : 쇠약한 사람의 경우에 선호
C. Hemorrhoids (치핵)
C1. Introduction
(1) 내외치핵정맥총(hemorrhoidal plexuses)가 과도하게 충혈, 탈출(prolapsed) 또는 혈전증이 된 것으로 변비와 배변 시 과도한 힘주기, 잦은 설사, 고령과 관련이 있다.
(2) 그 외 임신, 만성간질환 (문맥압상승, 정맥류형성)과 관련 있다.
(3) 내치핵(Internal hemorrhoids)
① 치상선(dentate line) 상방에 위치
② Superior rectal artery의 말단분지를 따라 종방향(longitudinally) 우측으로 후외측/전외측, 좌측으로
외측(2-, 5-, and 9-o'clock position)에 위치, 흔히 한 개면 5시 방향에 위치.

(4) 외치핵(External hemorrhoids)
① 치상선 하방에 위치
② Sensory innervation이 많은 anoderm으로 둘러싸여 있음. → 통증 야기
③ 아래(외)치핵 정맥 (inferior (external) hemorrhoidal veins) > 하대정맥(inferior vena cava)
C2. Clinical feature
(1) Hemorrhoidal bleeding
① 휴지에 묻어 나오거나 stool 표면에 이거나 배변 끝에 변기에 방울로 떨어짐.
② Most common source of anorectal bleeding
③ Massive hemorrhage은 흔하지 않음
(2) 통증
① 대개 외치핵 통증 (Unthrombosed인 경우 통 무통성)
② 내치핵 무통증 → Complication 생기면 아픔
③ 내/외치핵에서 unthrombosed 인 환자가 통증을 호소하면 perianal, intersphincteric abscess
or anal fissures 의심.
치질 비대는 변비 및 장기간의 배변, 잦은 설사, 고령과 관련이 있습니다. 복압이 증가하면 정맥의 역류가 방해되고 치핵 신경총이 울혈될 수 있습니다. 잦은 설사와 치질이 있는 환자의 경우 염증성 장 질환을 고려하세요. 치핵 정맥은 안정 시 압력이 높고 판막이 없을 수 있으며, 환자가 나이가 들어감에 따라 혈관을 둘러싼 지지 결합 조직이 감소합니다. 치질은 임신 중에 발생할 수 있으며 직장의 정맥 배액에 대한 지속적인 압력 증가의 결과 일 수 있습니다. Increased portal pressure, from chronic liver disease, may produce marked dilatation and varix formation, distinct from true hemorrhoids, resulting in bleeding that can be extremely difficult to control. Tumors of the rectum and sigmoid colon, often associated with constipation, tenesmus, and incomplete evacuation, may cause hemorrhoids. Although the most common cause of bright red rectal bleeding is hemorrhoids, tumors must be ruled out as a cause of rectal bleeding in patients >40 years of age. Ascites, ovarian tumors, distended bladders, and excessive fibrosis from radiation therapy may contribute to the formation of external hemorrhoids. Hemorrhoidal bleeding is usually limited, with the bright red blood on the surface of the stool, on the toilet tissue, or noted at the end of defecation, dripping into the toilet bowl. When patients describe the passage of blood clots, one should suspect colonic lesions. Chronic slow blood loss detected on fecal occult blood testing resulting in anemia requires further investigation. Hemorrhoids themselves generally do not cause pain unless they are thrombosed or are strangulated fourth-degree internal hemorrhoids. If the patient complains of pain, but on examination the hemorrhoids are not thrombosed, suspect perianal or intersphincteric abscesses or anal fissures. Thrombosed external hemorrhoids are painful and are often described as a burning perianal lump, and they usually exhibit a bluish-purple discoloration (Figure 85-6). Hemorrhoids may become more prominent with a Valsalva maneuver. As hemorrhoids increase in size, they may prolapse, requiring periodic reduction by the patient. Pain can be quite severe at the time of defecation and usually subsides with time.
Uncomplicated internal hemorrhoids are painless due to visceral innervation and lack of sensory innervation. Anoscopy reveals bulging, purple-colored veins at the distal rectum or anal canal (Figure 85-7). Often a chief complaint is painless, bright red rectal bleeding with defecation. Internal hemorrhoids may be palpable on digital examination when thrombosed or prolapsed.2 Nonreducible, prolapsed, internal hemorrhoids may become thrombosed and strangulated. They appear dark red, exhibit rectal bleeding, and cause exquisite pain and possibly urine retention. Ulceration, necrosis, gangrene, sepsis, and hepatic abscess formation may ensue. Internal hemorrhoids are classified by the amount of prolapse into the anal canal.
C3. Treatment
경증에서 중등도의 증상이 있는 1등급(치상선 위로 내강 돌출) 및 2등급(자연 감소를 동반한 탈출)의 내치질에는 따뜻한 목욕을 통한 보존적 치료가 종종 성공적입니다. 3등급(수동 축소술이 필요한 탈출증) 내치핵의 수동 축소술과 하루 세 번, 배변 후 15분 이상 온수 목욕(괄약근 압력을 감소시키는)이 가장 효과적인 증상 완화법입니다. 목욕 후에는 항문 주위 피부의 침식을 방지하기 위해 항문을 부드럽게 말리되 완전히 말려야 합니다. 국소 진통제와 스테로이드 함유 연고를 바르면 증상이 완화될 수 있습니다. 환자는 장시간 변기에 앉아 있지 말아야 합니다.대량 완하제와 대변 연화제는 급성기를 치료한 후에 사용해야 합니다. 변을 묽게 만드는 완하제는 항문염과 항문 패혈증을 유발할 수 있으므로 사용하지 마세요. 대량 완하제와 대변 연화제는 급성기를 치료한 후에 사용해야 합니다. 변을 묽게 만드는 완하제는 항문염과 항문 패혈증을 유발할 수 있으므로 사용하지 마세요. 증상이 있는 치질은 다양한 시술(경화 주사, 고무줄 결찰, 광응고, 냉동 요법, 전기 소작, 레이저 치료, 고주파 절제, 스테이플 수리 또는 절제)을 통해 확실한 치료를 할 수 있으므로 수술적 치료를 권장합니다. 치질 밴딩의 드문 합병증은 골반 패혈증입니다.2 외부 치질 치료는 증상의 정도에 따라 다릅니다. 혈전증이 48 시간 이상 존재하고 부기가 줄어들 기 시작하고 치질이 긴장되지 않고 통증이 견딜 수있는 경우 환자는 따뜻한 목욕과 대량 완하제로 치료할 수 있습니다. 항문 직장 고리 근방에 배치하는 좌약은 도움이 되지 않습니다.
반면에 혈전증이 급성이고 48시간 미만 지속되었으며 극심한 통증이 있는 경우 혈전 절제술로 상당한 완화 효과를 얻을 수 있습니다. 면역력이 저하된 환자, 어린이, 임산부, 문맥 고혈압 환자, 항응고제 복용 중이거나 응고병증이 있는 환자의 경우 응급실에서 혈전성 외치핵 절제술을 시행해서는 안 됩니다. 환자를 옆으로 눕거나 엎드린 자세로 눕혀서 최적의 노출을 확보합니다. 부피바카인 0.5%와 같은 국소 마취제, 에피네프린(1:200,000), 중탄산염 완충액과 함께 30게이지 바늘을 사용하여 절개할 표피 부위에 침투합니다. 타원형 절개를 통해 항문 가장자리 원위부 피부를 절개하면 혈전증이 노출됩니다. 절개 부위를 통해 혈전을 제거합니다. 혈전이 여러 개 있을 수 있으므로 타원형 절개를 통해 혈전이 있는 치핵의 지붕을 풀고 그 위에 있는 피부를 제거하는 기술은 단순히 절개하여 혈전을 제거하는 것보다 훨씬 더 나은 결과를 제공합니다(그림 85-8, A-D).
작은 거즈 조각의 모서리를 상처 부위에 집어넣고 몇 시간 동안 그대로 두어 출혈을 억제합니다. 거즈 바깥쪽에 작은 압박 드레싱을 붙이고 환자가 6~12시간 후 첫 번째 따뜻한 목욕을 할 때 제거할 수 있습니다. 오피오이드는 변비를 유발할 수 있으므로 급성 통증 조절에 필요한 최소 용량과 최단 기간 동안만 처방해야 합니다. 지속적인 출혈, 재발, 감염, 누공, 농양 형성 등의 합병증이 발생할 수 있으므로 24~48시간 후 추적 관찰을 권장합니다. 치핵 절제술은 신중하게 결정해야 합니다. 최근 소규모 연구에 따르면 급성 혈전성 내치핵 또는 외치핵 환자는 국소 니페디핀과 1.5% 리도카인 연고 또는 이소소르비드 디니트레이트 연고로 치료하고 수술 후 추적 관찰할 수 있다고 합니다..2,3
(1) Conservative therapy with warm bath
(2) Surgical consultation in the ED
Grade 4 incarcerated ① internal hemorrhoids
: Continued and severe bleeding / Pain / Incarcaration ± strangulation
(3) 외치핵에서 혈전증이 >48시간이면 존적 치료, 48시간 이내 혈전증은 극도로 통증이 심해
clot excision 필요.
(4) 응급실에서 excision 하지 말아야 하는 경우
① Immunocompromised patients ② Children
③ Pregnant women ④ Patients with portal hypertension
⑤ Anticoagulated tx. 하고 있는 환자 ⑥ Coaglupathy가 있는 환자

D. Anal fissures (항문열, 치열)
D1. Introduction
(1) 항문관 기시부 또는 치상선 아래에서 항문관을 따라 항문연(anal verge) 쪽으로 얕은 선형의 열상
(superficial linear tear)
(2) 통증이 있는 직장 출혈의 가장 흔한 원인, 소아와 young adult에서 흔하고 infants에서 직장 출혈의
가장 빈번한 원인
(3) Location : >90%에서 posteriorly midline에서 발생 (6시 방향)
D2. Clinical feature
(1) 갑자기 날카로운 통증이 배변 동안/배변 직후, 무딘 통증이 배변 후 수 시간 지속 가능
(2) 변비 동반된 경우 많음
(3) Child abuse 고려
(4) 소량의 선홍색 출혈, 통 휴지나 변에 묻어나옴.
D3. Treatment
(1) 증상 완화, anal sphincter spasm 완화, 협착방지
(2) 6주 내 healing이 되지 않거나 자주 반되면 surgical referral recommend
(3) Warm bath, topical lidocaine ointments and 1% hydrocortisone creams
E. Fistula-in-ano (항문루, 치루)
1.
치상선 부위 anal gland 감염으로 인한 abnormal inflammatory tract
2.
Clinical feature
(1) 지속적, 무통증, 혈액이 섞인, 점액성, 악취가 나는 분비물
(2) 농양 형성 시 throbbing pain이 지속되고 앉거나 움직이거나 배변 시 통증 심해짐
3.
Treatment
(1) IV fluids
(2) Analgesics
(3) Antibiotics (ciprofloxacin and metronidaxole)
(4) Antipyretics
(5) Surgical consulation
F. Anorectal abscess (항문직장 농양)
•
Anal gland orifice 막히면서 감염, 농양 형성
F1. 증상 : 통증, 화농성 분비물
F2. Location : Tintinalli 9th, p544, Figure 85-11


(1) Perianal abscess
Located close to the anal verge, posterior midline, ① as a superficial tender mass,
which may or may not be fluctuant
F3. Clinical features
(1) More common in early middle-aged male
(2) 배변 직전 악화, 배변 후 완화되지만 배변 사이에 지속되는 dull, aching, or throbbing pain
(3) 앉은 자세/활동 시 통증 악화, 뒤무직 동반
(4) 심해지면 기침/재채기 시에도 통증
F4. Treatment
(1) Perianal abscess : Incision (cruciate incision) and drainage
(2) All perirectal abscesses (supralevator, intersphincteric, and complicated ischiorectal)
① Should generally be drained in the operating room
(3) No packing, 만약에 한다면 loosely/not tightly. 24시간 이내 제거해야 한다.
(4) 다음 날부터 자주 warm bath 실시
(5) 건강한 환자에서 drainage 잘 된 경우에는 항생제는 필요 없다.
G. Proctitis
G1. Introduction
(1) 직장점막에 발생한 염증
(2) 원인
① 방사선치료 ② 자가면역,
③ 혈관염 ④ 허혈
⑤ 감염
(STD: Neisseria gonorrhoeae, Chlamydia trachomatis, Treponema pallidum, Herpes simplex
type 2, Human immunodeficiency virus, Human papillomavirus)
G2. Clinical feature
(1) 항문직장 통증 (2) 가려움
(3) 분비물 (4) 설사
(5) 출혈 (6) 하복부통증
G3. Treatment
(1) Stool softeners (2) sitz baths
(4) Careful anal hygiene, (3) Pain medications
(5) Antibiotics
•
Acute proctitis를 시사하는 증상/신체징후가 있는 모든 환자에서 gonorrhea, non-LGV chlamydia,
and incubating syphilis 제균이 시작되어야함.
H. Rectal prolapse
•
Mucosal prolapse/ Partial prolapse (incomplete) / Full thickness prolapse
H1. Clinical feature
(1) 통증이 저명한 증상이 아니며 부 불편감이 주증상으로 나타난다.
(2) 소아는 cystic fibrosis, polyps pelvic floor weakness, diarrhea, malnutrition 감별해야 함.
H2. Treatment
(1) Reduction : buttock을 양손으로 벌리고 손가락으로 서서히 탈장을 안으로 넣는다.
(2) Sugar : Prolapse된 부분 전체에 도포 15분 후 부종↓ → 정, 합성 감미료는 효과 X

I. Anorectal tumor
1.
Dentate line 기준으로 나뉜다.
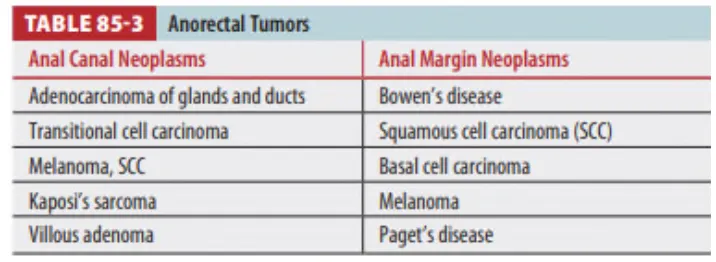
2. Anal canal은 피부, 눈 다음으로 melanoma가 잘 생기는 부위
J. Pilonidal sinus or cyst
1.
Painless cyst, acute abscess, chronic recurring cyst with draining sinus의 형태
2.
Infected pilonidal cyst는 종종 perirectal abscess로 오진될 수 있다
3.
Abscessed pilonidal sinus
(1) 거의 항상 sacrum과 coccyx 상방 posterior midline에 위치
(2) Anorectum과 연결되지 않음
4.
Carcinoma는 chronic, recurrent pilonidal sinus의 드문 합병증
(1) 남성에서 더 흔함
5.
Treatment
(1) Incision & Drainage, antibiotics는 cellulitis가 있을 때 투여
(2) Midline의 측면에서 longitudinal incision → Debris 재축적 방지, Midline 염증반응 최소화

