
.png&blockId=a4d3b3b4-055b-4aac-8427-dd932bd026b1)
A. Introduction
1.
Visual pattern 인식이 진단의 핵심
a.
ED로 내원하는 피부질환은 주로 infections, irritants, allergies
2.
주증상 확인
(1) 간략한 history (duration, rate of progression, location of lesions)
(2) Dermatologic examination 시행 (morphology, distribution)
(3) 감별질환 고려
(4) 추가 정보 병력 청취 (associated complaints, comorbidity, medication, exposure)
(5) 필요 시 피부과 consult 또는 외래예약
B. Diagnostic approach
B1. History
•
Morphology, evolutionary nature, rate of progression and distribution에 대해 파악
•
동반된 전신 증상에 대해 청취
① Exposures ② Immunization ③ Toxins ④ Chemicals
⑤ Foods ⑥ Animals ⑦ Insects ⑧ Plants
⑨ Ill contacts ⑩ Sexual history ⑪ Medical & family hx ⑫ Occupation
⑬ Travel
•
불편함의 정도를 사정 ex) Painful dermatitis → red flag sign; no self-limiting lesion
B2. Examination
(1) 모든 skin, mucosal surface 시진
•
hair, nails, scalp, mucous memb. etc.)
•
Distribution, pattern, arrangement, morphology, extent, and evolutionary changes
◦
Distribution : skin finding의 위치, 분포
◦
Pattern : 해부학적, 기능적, 생리학적 배열
ex) 흉부의 일측성 band like arrangement : varicella zoster를 시사
•
Burn에 사용하던 Rule of nine을 이용하여 skin involvement 정도를 측정
① topical medication의 양을 정하거나, oral medication이 더 적절한지 결정.
② 광범위한 (>90% of BSA) erythroderma (홍피부증)는 피부과적 응급
: Severe infectious dermatitis / Toxic shock syndrome / Cutaneous T-cell lymphoma/Drug reaction / Psoriasis / Seborrheic dermatitis
•
Lesion arrangement
① Symmetry and configuration
② Bilateral symmetry는 systemic internal event 또는 symmetric external exposure
③ Configuration 배열이 single lesion인 경우 그 병변의 feature를 참고해야 한다
분포와 패턴 | 감별진단 |
굴곡부 | 아토피 피부염, 칸디다증, 습진, 비늘증(ichthyosis) |
햇빛 노출 부위(얼굴, 상부 흉부, 원위 사지) | 일광화상, 광과민성 약물 발진, 광과민성 피부염, 전신성 홍반루푸스, 바이러스 발진, 포르피리아 |
원위 사지 | 바이러스 발진, 아토피 또는 접촉성 피부염, 습진, 로키산홍반열, 임균혈증 |
흉부 전후면 | 장미색 비강진, 이차 매독, 약물 발진, 아토피 또는 접촉성 피부염, 건선 |
옷으로 덮이는 부위(흉부와 하지 원위부) | 접촉성 피부염, 건선, 모낭염 |
여드름양 분포(얼굴과 상부 흉부) | 여드름, 약물 유발 여드름, 자극성 피부염 |
용어 | 설명 |
원형성(Annular) | 고리 모양이거나 병변의 가장자리에 해당함 |
활상(Arcuate) | 활 모양의, 굽은 형태 |
환상(Circinate) | 원형의 |
융합성(Confluent) | 서로 융합하여 하나로 뭉치는 |
피부분절성(Dermatomal) | 띠 모양이거나 해부학적 피부분절에 따라 몸의 한쪽에 국한 |
원반형(Discoid) | 단단하고 둥글며 약간 융기된, 원반 모양의 |
분리성(Discrete) | 서로 떨어진, 개별적인 |
군집성(Grouped) | 무리지어 모여 있는, 군집된 |
점적성(Guttate) | 산재한, 물방울처럼 흩어진 |
나선성(Gyrate) | 소용돌이치듯 꼬이거나 구불구불한 |
헤르페스양(Herpetiform) | 기어가듯 퍼지는, 포행성 |
홍채형(Iris) | 동심원 모양 |
선상(Linear) | 일렬로 배열된, 선 모양의 |
다환성(Polycyclic) | 겹치는 원들이나 불규칙 곡선의 경계 |
망상(Retiform) | 그물 모양의 |
뱀행성(Serpiginous) | 뱀처럼 구불구불 기어가듯 퍼지는 |
•
Morphology
① 초기 병변을 인식하는 것은 진단에 매우 중요.
② Primary lesion
: 치유, 감염, 약물투여, 긁기 등의 2차적 문제로 변경되지 않은 병변.
(macules, papules, nodules, tumors, cysts, plaques, wheals, vesicles, bullae, pustules)
③ Secondary lesion
: 외부 인자들에 의해서 외관이 변형 (crust, scales, fissures, erosions, ulcer, excoriations...)
•
사진들은 Tintinalli p1608. Table 248-3,4,5 참조




C. Diagnostic techniques
C1. KOH preparation
•
Molluscum contagiosum & dermatophytic 감염 의심 시
•
Skin scales, nail parings, subungual debris, short residual hairs 에 시행
C2. 현미경 검사
•
Scabies and lice(louse, 이) 의심 시 현미경적 분석이 중요
•
피부 검체의 donor site 선정이 매우 중요함 (best site는 손가락, 손목, 팔꿈치의 papule)
C3. Tzanck smear
•
blistering disorder (herpes simplex, herpes zoster, varicella)
C4. Wood‘s light examination
(1) Erythrasma (a superficial Corynebacterium infection of moist skin in the groin, axilla, and
web spaces), fungal infection, certain pseudomonal skin infection, porphyricutanea tarda
감별에 유용
(2) 365nm파장의 자외선 이용
C5. Ancillary studies
D. ED Treatments
D1. Systemic corticosteroids
(1) 잠재적 적응증
•
Urticaria
•
Angioedema
•
Toxicodendron dermatitis (rhus, poison ivy, or poison oak)
•
Other contact or allergic disorders
(2) 피부과와 상의 후 사용해야 하는 경우
•
Erythema multiforme, toxic epidermal necrolysis, vasculitis
(3) Relatively contraindication
•
Diabetes
•
Hypertension
•
Active peptic ulcer disease
•
Psychiatric disease
•
Immunodeficiency
(4) 거취
•
Follow-up within 2 to 3 days with the primary care physician or a dermatologis
•
Severe disease의 경우 경구 스테로이드로 12~24시간 내 상당한 경감을 보인다.
•
Poison ivy or oak eruptions 시 Prednisone (1mg/kg) with a slow 2- to 3-week taper
(Rebound dermatitis를 피하기 위해)
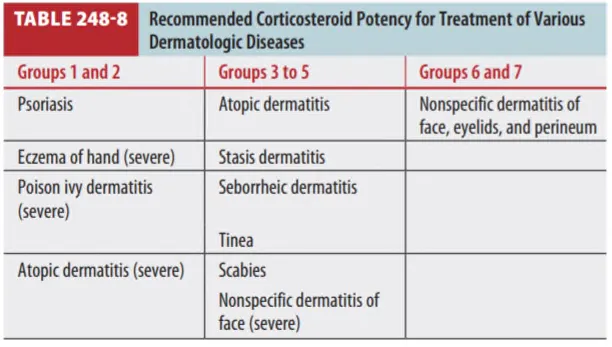
D2. Topical corticosteroids
•
가장 강력하고 유용
•
Vasoconstriction 능력에 따라 potency 구분
◦
Group1 세고, Group7 약함 (Table 248-7 참조)
◦
Ointment > creasms or lotions
•
대부분이 fluorination(불소첨가) 되어 potency 증가.
But, adverse reaction risk 높아짐 → Fluorinated formulation은 임산부에 금기
•
Hydrocortisone (group7) : 1%~2.5%, 소아에도 안전, 일반적으로 많이 쓰임
→ 얼굴, 외음부, 굽힘 부위 등 (손발은 두꺼워서 침투 X)
•
Triamcinolone acetonide & fluocinolone acetonide : 중간 potency
→ 두피, 몸통, 폄 부위, 손발바닥 (얼굴, 외음부, 소아에 사용 금지)
(1) Application of topical steroids
•
간단하다 씻고 바를 필요 없고, 바르고 나서, 마사지 해준다.
•
임의로 약을 더 바르거나 줄이거나 하는 것은 옳지 않다.
•
최적의 용법은 대부분 결정되어 있지 않음.
(2) 바르는 스테로이드 용량 결정 (어렵다)
•
Burn rule of nines 이용하여 체표면적 계산
•
구해진 체표면적(%) X 30 = 1번에 바르는 양. gram. (A)
•
하루에 바르는 횟수 X 치료 일수 = 총 바르는 횟수 (B)
•
처방해야 하는 total grams = A X B
(3) Tachyphylaxis
•
Enzyme-mediated event로 약물의 효과 감소. 내성.
•
Tachyphylaxis 피하기 위해서 interrupted application schedule 적용
(ex 2주(하루 3회) 사용 후 1주 쉬고 다시 반복)
D3. Antihistamine
(1) Antihistamines (Histamine-1 antagonists) : 가려움 조절 시 사용
① 1세대 : Diphenhydramine and hydroxyzine / PO, IM, or IV
② 2세대 : Astemizole, cetirizine, fexofenadine, loratadine / 사용 횟수, 진정작용 감소. 비싸다.
→ 용량 증가시켜 사용하는 것은 side effect 증가, 가려움 조절이 더 잘되지는 않음
(2) Topical antihistamine preparations : 추천되지 않음
(3) Histamine-2 antagonists (ranitidine or famotidine)
① Allergy-mediated event, in particular urticaria
② H-1 antagonist와 병합하여 사용.
D4. Antimicrobial agents
(1) Wound dressing의 보조제, 일차적 치료로는 사용되지 않음. (예외 Impetigo : Mupirocin)
(2) Wound dressing 일반 약제 : polymyxin B, bacitracin, neomycin, and silver sulfadiazine
(3) Silver sulfadiazine은 착색되니까 얼굴에 사용하지 마라!
(4) 아프타성 구내염 : tetracycline rinse
D5. Non-antimicrobial topical agents
“If it’s dry, wet it, and if it’s wet, dry it”
(1) Creams
① 가장 다용도
② 급성기 치료에만 사용
③ 지속적 사용 시에는 excessive drying.
④ 들어있는 방부제에 allergy 있는 사람이 있음 → 연고제로 바꿔 처방.
(2) Ointments
① 폐쇄성이며 cream보다 더 깊이 침투.
② Acute exudative syndromes & intertriginous areas of the body에는 스테로이드 연고 X
(3) Gels
① Alcohol-containing gels : best for acute exudative lesions
② Alcohol-free combinations : dry, scaling conditions
(4) Solutions or lotions : 잔류물을 남기지 않으므로 두피 및 다른 모발부위에 유용
