

조기재분극증후군(Early Repolarization Syndrome, ERS)은 심전도(ECG)에서 조기재분극 패턴이 나타나면서 치명적인 부정맥(심실세동 등)이 발생하거나 돌연사로 이어진 경우를 의미합니다. 이 패턴은 예전에는 무해한 양성 변이로 여겨졌으나, 2000년대 이후 연구를 통해 일부 환자에게서 심실세동 및 급성 심장사와의 연관성이 확인되면서 '증후군'으로 명명되었습니다.
주요 특징
•
심전도(ECG) 소견: 심전도 상 J점(QRS파의 끝과 ST분절의 시작점이 만나는 지점)이 기준선보다 상승되어 나타납니다. 이는 QRS파의 끝에 물결 모양(notch) 또는 뭉툭한 형태(slur)로 나타날 수 있으며, ST분절의 상승이 동반되기도 합니다.
•
발생 위험: 전체 인구 중 조기재분극 심전도 패턴을 보이는 사람은 1~13%에 달할 정도로 흔하지만, 이들 대부분은 아무런 증상이 없고 부정맥 위험도 낮습니다. 그러나 특정 심전도 양상(아래쪽 또는 옆쪽 유도에서 J점 상승)을 보이면서 심실세동 병력이 있는 환자들은 위험도가 더 높습니다.
•
주요 원인: 심장 내 이온 채널의 기능 이상으로 인해 심장 재분극 과정에 문제가 생기는 '이온 통로병증(channelopathy)'이 원인일 수 있습니다. 일부는 유전적 요인과 관련이 있지만, 모든 사례에서 유전자가 밝혀진 것은 아닙니다.
증상과 치료
•
증상: 대부분의 조기재분극 환자는 무증상입니다. 그러나 치명적인 부정맥이 발생할 경우, 실신이나 심장마비와 같은 심각한 증상이 나타날 수 있습니다.
•
진단: 심전도 검사가 가장 중요하며, 심실세동 병력과의 연관성을 종합적으로 고려하여 진단합니다.
•
치료:
◦
무증상 환자: 심전도상 조기재분극 패턴만 있고 증상이 없는 환자는 일반적으로 특별한 치료가 필요하지 않으며 경과를 관찰합니다.
◦
고위험 환자: 증상이 있거나 위험도가 높은 환자의 경우, 삽입형 제세동기(ICD) 시술이 고려될 수 있습니다. ICD는 위험한 부정맥 발생 시 전기 충격을 주어 심장 박동을 정상화하는 장치입니다.
주의 사항
•
전문가 상담: 조기재분극 패턴이 심전도에서 발견되었다면, 부정맥 전문의와 상담하여 정확한 위험도를 평가하고 필요한 경우 적절한 조치를 취해야 합니다.
•
일반적인 조기재분극과의 구분: 조기재분극 패턴 자체는 흔하게 발견되는 무해한 소견일 수 있으므로, 조기재분극 '증후군'과의 구분이 중요합니다.
“Benign” Early Repolarization: A misnomer predicting idiopathic VF
(Benign) early repolarization was present in 31% of patients resuscitated after cardiac arrest due idiopathic ventricular fibrillation (VF), compared with 5% of control subjects. This pattern was present on all case subjects in whom pre-existing ECGs were available.
In 2008, Haïssaguerre et al challenged the well-embedded term “benign” early repolarization by demonstrating a link between this familiar ECG pattern and idiopathic VF arrest
•
Standard patterns of QRS-ST junction elevation > 1mm in inferior or lateral leads were found to be present in 31% of patients with idiopathic VF, with an odds ratio of 10.9 compared to control subjects
•
Findings gave weight to previous experimental studies which had shown than BER predisposes to potential arrhythmogenicity but for which very limited supporting clinical evidence had been demonstrated
•
Other smaller case studies have demonstrated an incidence of BER in patients with idiopathic VF of up to 60%
Le Syndrome de Haïssaguerre (idiopathic VF):
Diagnosis of exclusion in patients who have survived a VF episode without any identified structural or metabolic cause despite extensive diagnostic testing.
Early Repolarisation Syndrome (ERS)
ERS refers to the presence of a BER pattern in patients who have survived idiopathic VF. Given the higher incidence of idiopathic VF in patients with BER, the term may be more of an observation than a separate entity.
In 2011, Antzelevitch et al described different types of ERS that correlate to ECG regions of BER and their correlation to risk of recurrent VF
ERS | BER pattern | VF recurrence |
Type 1 | Lateral precordial leads | Low; prevalent among healthy male athletes |
Type 2 | Inferior leads | Moderate |
Type 3 | Global | High; association with VF storms |
In 2012, Junttila et al proposed a further classification of early repolarization (ER) patterns. They defined two types of J-point elevation:
1.
Benign form: J-point with rapidly ascending ST segment
2.
Malignant form: J-point with horizontal or descending ST segment
A. Benign type with rapidly ascending ST and
B. Malignant type with horizontal variety of ER.Source: Sethi et al 2014

The electrophysiology
Idiopathic VF requires a triggering ectopic, usually short-coupled PVCs, and a maintenance substrate
•
When identifiable, 80-90% of triggering ectopics originate from the Purkinje system or neighbouring structures (moderator band, papillary muscles)
•
VF requires the continuous formation of reentry for its maintenance, often which is localised to a myocardial region with identifiable structural abnormalities (fibre arrangement, fibrosis). Idiopathic VF patients would be expected to have uniform reentries on electrode mapping, however when studied they also demonstrate clustering of reentries, indicting “microstructural” defects
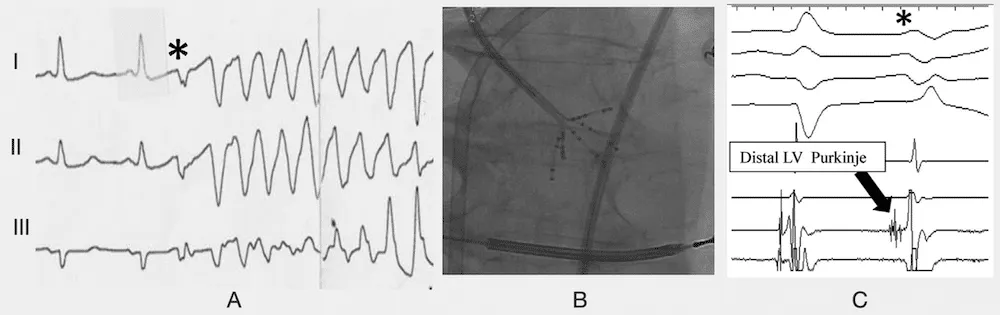
Patterns of Purkinje activity in patients with VF: Haïssaguerre 2019(A) Typical short-coupled ectopy(*) initiating VF.(B) Multielectrode mapping with a multispline catheter recording(C) the earliest activity preceding ectopic beat in the distal left posterior fascicle
Clinical significance
Awareness of the correlation between BER and idiopathic VF likely lies more in preventing and treating recurrent episodes of VF, as follow up of case subjects found a higher incidence of recurrent VF. Although ICD is the treatment of choice, additional drugs may be required to prevent recurrent episodes and treat VF storms. Follow-up of patients with idiopathic VF found isoproterenol infusion the only drug reliable in treatment of VF storms, and quinidine of most benefit in preventing recurrence.
Size of J-point elevation on initial ECG displayed correlation with the number of recurrent VF episodes, with greater than 50 recurrent episodes in the three subjects with the highest J-point elevation (> 5mm). Despite this, given the prevalence of the BER pattern in the wider community, current recommendations remain that asymptomatic patients with J waves not undergo further testing.
Limitations
Subsequent studies affirming findings by Haïssaguerre et al have involved smaller patient populations, and although they confirm the link between BER and idiopathic VF, they do not allow us to discern which patients with ECG findings of BER are at risk of an initial episode of idiopathic VF. The benign natural history for most patients with BER and its prevalence among young individuals suggests other specific ECG markers are required to determine which patients would benefit from electrophysiological testing. This may include further research into types of ERS, in particular type 3 ERS with a global BER pattern, and its correlation to idiopathic VF.
