
•
Alertness와 responsiveness가 감소되어 깨어날 수 없는 상태
•
병태생리 : Neuronal function에 필요한 substrate의 결핍(hypoglycemia or hypoxia)
D1. 평가도구
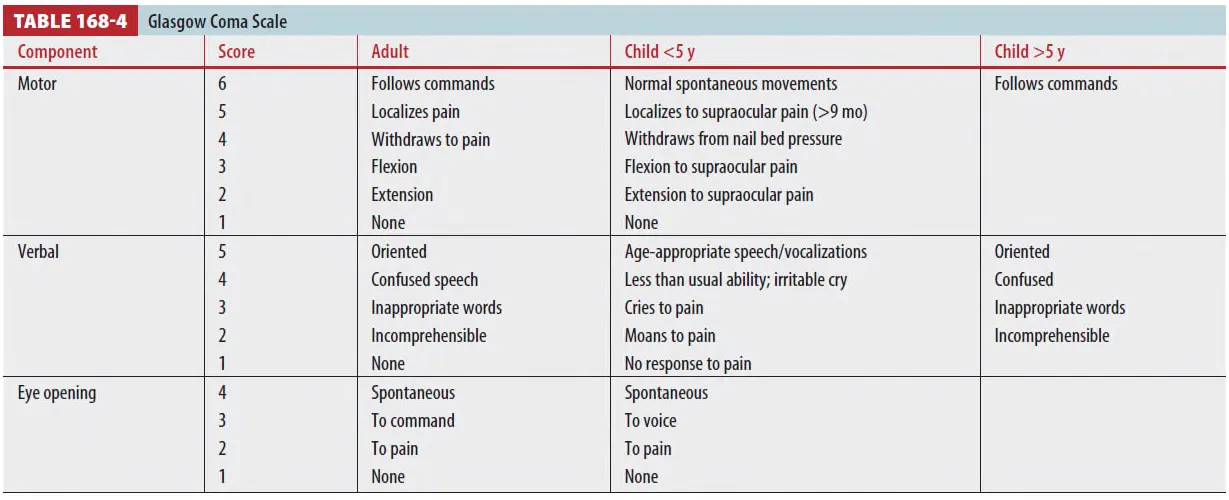
(1) GCS score
: 의식변화에 대해 임상적으로 점수 매기는 체제
•
Advantage
◦
간단하고 verbal, motor, eye-opening function을 구분하여 평가할 수 있음
•
Disadvantage
◦
Hemiparesis나 다른 focal motor sign에 대한 인지 부족
◦
고급 인지 기능에 대한 평가가 안 됨
◦
평가자 간 차이가 있다
(2) The FOUR(Full Outline of UnResponsiveness) score
•
ICU에서 사용
•
Advantage
◦
Eye and motor responses 뿐만 아니라 간단한 brainstem function &
respiratory pattern 평가 가능
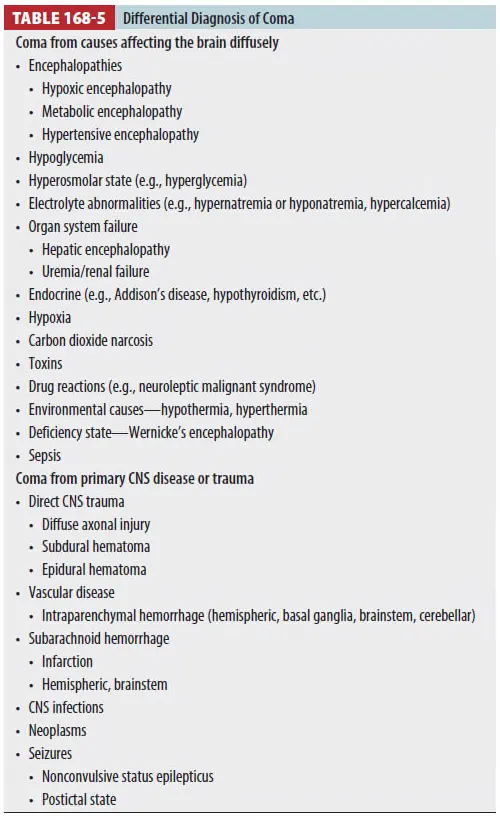
D2. Cause
(1) Primary CNS cause
•
Brainstem disorder나 bilateral cortical dysfunction으로 인해 발생
•
Unilateral hemispheric disease(stroke)로는 coma 상태 빠지지 않는다
(2) Herniation syndrome
•
Uncal herniation syndrome
: Medial temporal lobe이 upper brain stem 을 압박한 결과 의식저하가 점차 진행하여 반응이
사라짐,
: Medial temporal lobe이 3번 뇌신경을 압박하여 동측의 동공반사가 sluggish하게 있다가
확장되고 반응이 사라지게 된다.
: 반대측 cerebral peduncle에 있는 descending motor tracts 을 누르기 때문에
•
Central herniation syndrome
: 점진적인 의식소실, brainstem 반응 소실, decorticate posturing, irregular respiration
: Mechanism
Midline shift without herniation → Local cerebral edema or local IICP
→ vascular compression
(3) Diffuse increased ICP는 diffuse CNS dysfunction을 유발한다.
•
CPP=MAP-ICP, MAP 50~100mmHg에서 cerebral blood flow가 유지된다
•
ICP가 조절되지 않고 극도로 상승하면 brain ischemia 유발된다
D3. 임상 양상
•
Coma의 depth와 원인에 따라 다른 양상
ex) hemispheric hemorrhage에서 midline shift 있는 coma
•
Hemorrhage와 surrounding edema가 늘면 ICP 상승하거나 brainstem compression이 유발
→ Motor tone이 완전히 상실되거나 ocular finding이 사라질 수 있다
(1) Toxic metabolic coma
•
Diffuse CNS dysfunction → Lack of specific region of brain dysfunction
•
만약 환자가 자발적인 움직임이나 반사를 보인다면 반신마비 없이 대칭적임.
•
전형적으로 작지만 일반적으로 동공반사는 보존, 대칭적 외안 운동
•
Barbiturate 중독은 예외적으로 large, extraocular movements absent, muscles flaccid, and
the patient apneic (brain death 와 같은 모습)
(2) Coma from supratentorial lesion - ex. uncal herniation syndrome
•
Progressive hemiparesis or asymmetric muscle tone and reflexs
•
자극에 대한 asymmetric response or asymmetric extensor or flexor posture
•
Large acute supratentorial lesion은 temporal lobe herniation와 일치하는 양상이 없다
•
ICP 상승 → Cerebral perfusion 감소해 lateralizing sign 없이 Coma, Cushing reflex
(hypertension, bradycardia)
(3) Coma from infratentorial lesion
•
Expanding lesion (cbll. hemorrhage or infarction)
•
Abrupt coma, abnormal extensor posturing, PLR과 extraocular movement의 loss
•
Early brainstem compression의 경우 brainstem reflex 소실이 빠르게 진행함
•
Pontine hemorrhage의 경우 pinpoint-sized pupil 양상 보임
(4) Pseudocoma
•
적절한 병력 청취와 자극에 대한 반응을 관찰.
•
PLR, EOM, muscle tone, reflex → Intact
•
환자가 검사자를 보지 않으려는 주시 회피
•
칼로리 검사에서 안진이 있다면 생리학적이 아니거나 무반응 하는 척
D4. 진단
•
안정화, 진단, 치료행위가 동시에 이루어진다. 가능한 모든 Hx. source 찾아내야 한다.
•
진찰, lab, neuroimaging을 통해 응급실 거의 모든 환자의 coma 원인을 찾을 수 있다
•
Coma의 reversible cause도 고려해야 함 (저혈당, opiate overdose)
•
Coma의 onset의 tempo → 중요한 진단적 가치를 가짐
◦
Abrupt coma : abrupt CNS failure (catastrophic stroke or seizure) vs
◦
Slowly progressive onset : progressive CNS lesion (tumor or SDH)
(1) General examination and measurement of V/S
→ Trauma의 sign이나 다른 원인을 제시
(2) Neurologic test
•
Cranial n. exam, corneal reflex, oculovestibular reflex 통해 focal CNS lesion을 시사
•
Abnormal extensor or flexor posture는 profound dysfunction을 시사
•
Physician의 목표는 CNS dysfunction이 diffuse brain impairment에서 오는지 아니면
focal lesion에서 sign이 보이는 것인지를 빠르게 결정하는 것이다.
(3) CT scanning
→ The neuroimaging procedure of choice
(4) Lumbar puncture
→ CT 소견이 불명확하거나 CNS bleeding or infection 의심 시
(5) Basilar artery thrombosis
•
Head CT에서 hyperdense basilar artery외에 normal 소견을 보이는 comatose patient에서 의심
•
MRI or cerebral angiography
D5. Special considerations in coma
(1) Pediatric
•
toxic ingestion, infection, abuse가 훨씬 많고 중요
(2) Nonconvulsive status epilepticus
•
전신발작 후에 unresponsive 유지될 때는 motor movement는 없지만 electrical seizure 상태가 지속되는 것일 수 있다.
•
Seizure가 멈춘 후에 30분 이내로 의식이 회복되지 않는다면 nonconvulsive status epilepticus를 고려하고 신경과 consult & EEG 시행해야함.
D6. 치료
•
원인 규명과 그에 맞춘 구체적인 치료를 시작해야 함.
•
A-B-C 평가.
•
Hypoglycemia & opioid toxicity 같은 reversible cause 평가하고 치료.
(1) Antidotes
•
원인 모르는 coma에 flumazenil은 비추천
•
Naloxone은 유용(opiate overdose 징후 없기도 함)
(2) ICP 상승
•
Paralysis와 sedation drug 자유롭게 사용.
•
30도 head elevation 유지
•
Osmotic diuresis (mannitol 0.5~1.0g/kg) 투여
•
Dexamethasone 10mg IV (tumor edema)
•
Hyperventilation 통한 PaCO2감소 : Cbr. blood volume 줄여 ICP 하강
(현재 brain injury 후 첫 24시간은 과호흡 (PaCO2<35mmHg) 피해야)
D7. Disposition and follow-up
•
Reversible cause 의해 발생한 coma (eg. insulin-induced hypoglycemia)경우 귀가 후 F/U
•
지속적으로 altered consciousness의 경우 입원치료
