A. Introduction
1.
Aneurysm
(1) 정상 arterial wall diameter의 1.5배 초과로 늘어난 것
(2) True aneurysm : vessel 전층을 involve
(3) Pseudoaneurysm : vessel wall의 일부를 포함
2.
위험인자
(1) Smoking (2) 고령 (3) 백인
(4) 고혈압 (5) 고지혈증 (6) 결체조직 질환
(7) 가족력
B. Pathophysiology
1.
점차적으로 vessel 내 elastin, collagen, fibrolamellar unit이 감소하면서 vessel wall의 media 얇아짐
→ Tensile strength가 감소
→ Wall이 늘어나면 Laplace law에 따라 wall tension이 증가해 더 크고 빠르게 늘어남.
2.
SES가 낮은 환자군에서 aneurysm이 rupture되어 확인되는 경우가 더 많아 예후도 안 좋다.
3.
Mycotic aneurysm vs infected aneurysm
(1) 모두 vessel wall에 infection으로 인해 발생. IV drug abuse에서 많이 발생하므로 의심해야 함.
(2) Mycotic aneurysm : septic emboli으로 인해 2차적으로 aneurysm이 발생
(3) Infected aneurysm : aneurysm에 infection이 발생한 것
4.
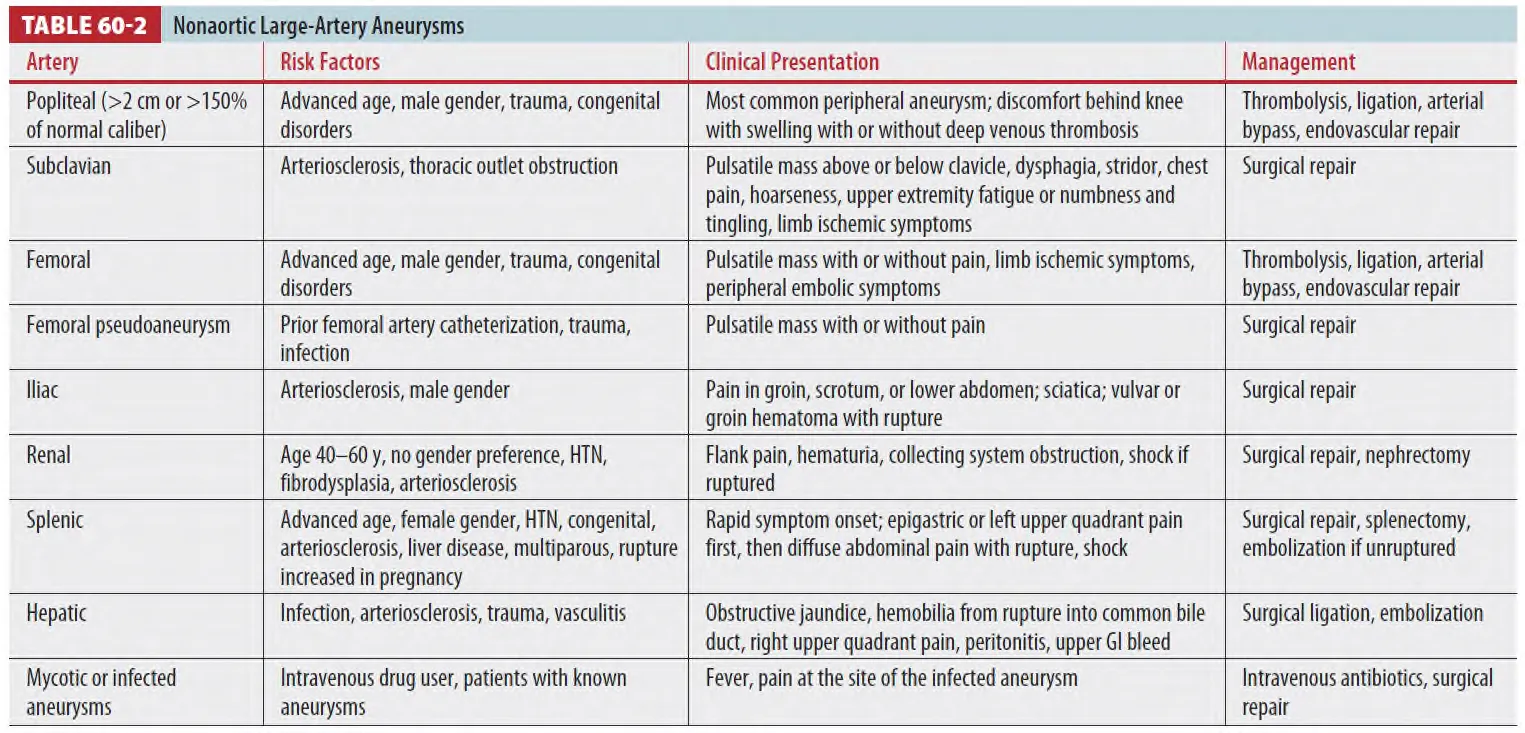
Peripheral and visceral aneurysm
(1) Popliteal a.가 가장 흔한 peripheral aneurysm. Femoral a.는 uncommon.
(2) Visceral a. an.은 어디에나 발생하지만 renal, splenic, hepatic a. 에 흔함
(3) Rupture 시 80% mortality rate, thrombosis시 perfused organ의 ischemia
C. General clinical features of aneurysms
1.
임상 양상과 증상이 non-specific; 위치, mass effect, distal ischemia에 따라 차이가 있다.
2.
Visceral aneurysm은 abdomen, flank complaint로 시행한 APCT에서 종종 확인되고
lower ext. aneurysm은 DVT w/u으로 시행한 ext. Doppler US에서 확인된다.
D. Symptomatic abdominal aortic aneurysms
•
AAA: 3cm 이상일 때 진단, 5cm 이상일 때 repair 고려
•
대부분 >60세, 가족력, 남성, 다른 arterial aneurysm등의 병력이 위험인자
1.
Clinical features
(1) 등 통증, 복부 통증이 m/c symptom; Severe, abrupt in onset, ripping or tearing pain.
(2) The classic triad (ruptured AAA)
① 복통 ② 박동성 복부 종괴 ③ 저혈압
•
하지만 1/3 정도의 환자에서 확인됨.
(3) 이외 syncope, non-classic site pain(flank, groin, isolated quadrant of abdomen, hip),
nausea, vomiting, bladder pain, tenesmus 등의 증상이 있음.
(4) Aortoenteric fistula로 인한 GI bleeding, extremity ischemia, hemorrhagic shock,
sudden death 발생 가능
(5) 심한 복통, 등 통증 후 발생한 실신의 경우 aneurysmal rupture일 수 있음.
2.
Diagnosis
(1) 임상적으로 의심해 영상학적으로 진단
(2) 신체진찰만으로 동맥류를 진단, 배제하기 힘들다.
① Aneurysm의 압통은 expansion, rupture를 시사.
② 비만한 경우 신체진찰이 어렵고 마른 경우 aortic size가 과대평가될 수 있다.
(3) Hypotension, tachycardia는 환자군 중 소수에서 관찰된다.
(4) 실신, 복통, 흉통, 등 통증에 대한 다른 질환과의 감별이 필요. (심장, 복부, 후복막강, 신장, 간담췌)
(5) 동반질환의 각 증상이 진단을 모호하게 할 수도 있다. (Coronary artery disease, COPD 등)
(6) Acute rupture에서 periumbilical ecchymosis(Cullen sign), flank ecchymosis (Grey Turner
sign) 같은 external sign은 드물다.
(7) Retroperitoneal blood가 perineum, groin 등으로 들어가 scrotal or vulva hematoma,
inguinal mass 등이 생길 수 있고 psoas m.을 자극해 iliopsoas sign이 나타나거나 femoral n.를
압박해 neuropathy가 발생할 수 있다.
(8) 설명하기 어렵거나 대량의 GI bleeding의 경우 aortoenteric fistula를 고려해야 함.
→ Aortovenous fistula가 발생할 수 있고 이로 인해 high output heart failure가 발생할 수 있다.
3.
Imaging
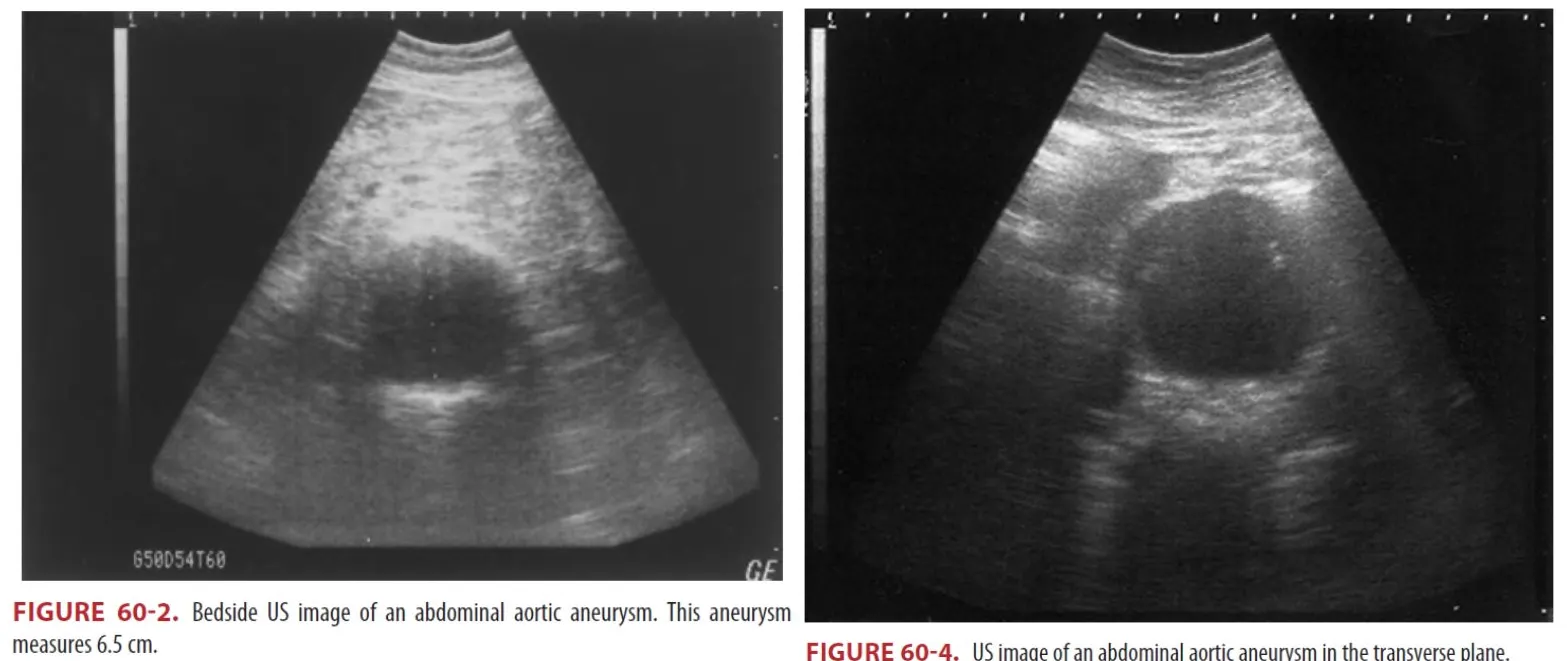
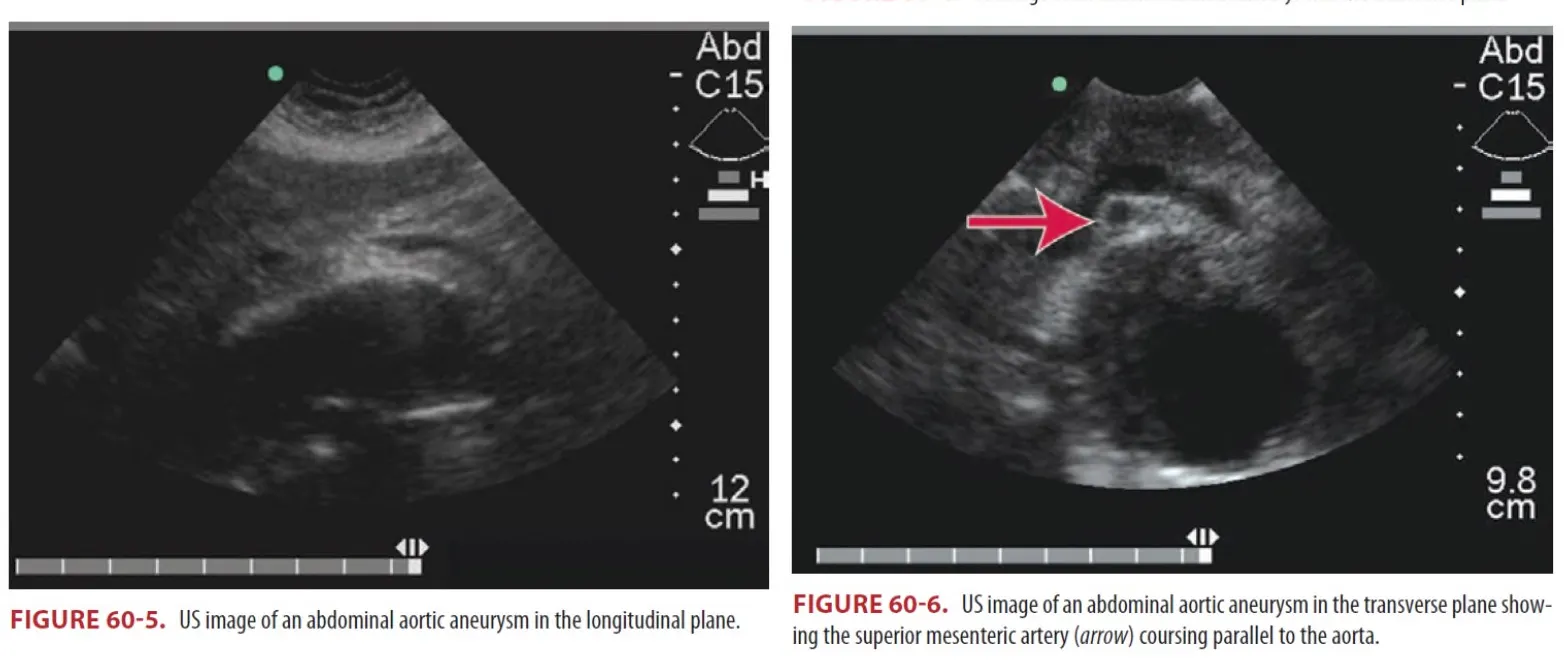
(1) Unstable한 환자의 경우 응급실을 나가서는 안 되고 bedside US가 image of choice이다.
① Bedside US는 ideal initial screening.
② Aneurysm을 확인하고 크기를 평가하는데 90% 초과의 민감도를 가짐
③ 3cm 미만의 aortic diameter는 acute aneurysmal disease를 배제할 수 있다.
(2) Stable한 환자의 경우에서 abdominal aneurysm이 의심될 때는 US, CT or MRI를 시행.
① 조영제를 사용한 CT는 동맥류 및 관련된 출혈을 가장 자세하게 확인할 수 있어서
모든 stable한 abdominal aneurysm 의심 환자에서 CT를 진행한다.
(3) Plain abd. films에서는 석회화와 bulging aortic contour 소견이 보일 수 있다.
D4. Treatment of AAA
(1) 무증상 AAA
•
크기가 작아도 follow-up이 필요하다
•
≥ 5cm (outer~outer wall)은 rupture risk가 증가해 수일 내 혈관전문의 follow up 필요함
•
증상 악화나 실신 발생시 즉시 응급실 재내원하도록 교육
•
여성, 임산부, 산욕기 여성은 rupture risk 증가.
◦
5.5cm보다 작을 경우 repair 하는 것이 남성의 경우 survival rate에 변화가 없으나
여성의 경우 고려되기도 한다.
•
Endovascular aortic repair(EVAR)가 asymptomatic AAA에서 고려되기도 한다.
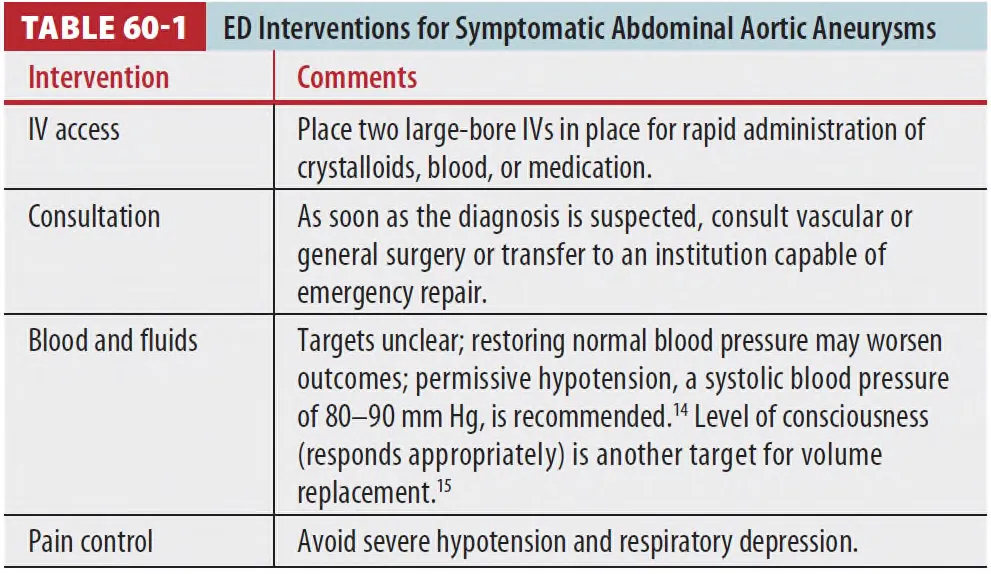
(2) 증상이 있는 AAA
•
증상이 있으면 크기와 상관없이 응급상황으로 고려하고 surgical consultation이 필요함.
•
무증상과 비교해 증상이 있는 경우 2배, rupture의 경우 7배 perioperative mortality가 높다.
•
크기가 증가, 심한 고혈압의 경우 esmolol을 추천 (Target: sBP 120mmHg)
•
REBOA 또한 고려 가능하나 연구가 부족하고 시행 가능한 병원이 제한적이다.
Ⅴ. Thoracic aortic aneurysms
1.
직접 주변 구조를 누르거나 침식시켜 fistula가 형성될 수 있다.
2.
Fistula가 형성될 경우 rapid resuscitation 없이는 fatal
3.
Asymptomatic 한 경우 BP control하며 refer한 뒤 추후 open or endovascular method로
처치를 고려한다.
Ⅵ. Extremity and visceral aneurysms
1.
Expansion이나 rupture로 증상을 일으킨다.
2.
Popliteal aneurysm : P/E상 firm, pulsatile mass. US로 진단, bilateral 가능성 → 양쪽을 확인
3.
Hepatic a. aneurysm : Quincke’s triad (jaundice, biliary colic, upper GI bleeding)