
Ⅰ. Acute kidney injury
1.
신장기능의 급격한 소실을 의미
2.
Kidney Disease: Improving Global Outcomes (KDIGO) 로 단계 구분

1.
AKI는 주로 3가지 prerenal, renal, postrenal로 나눌 수 있다.
(1) Prerenal : m/c
① 불충분한 renal perfusion으로 발생.
② Hypovolemia (bleeding, vomiting, diarrhea)
③ Effective circulation 감소 (heart failure, cardiogenic shock, septic shock)
(2) Renal
① Renal parenchyme의 구조적 손상으로 발생
② Glomerular dz (APN, Nephrotic syndrome, GN)
③ Vascular dz (HUS, Thrombosis, Vasculitis), interstitial dz
(3) Postrenal
① Lower urinary tract의 obstruction으로 발생
② Ureter stone, renal vein thrombosis, urethral obstruction
Ⅱ. Diagnosis
1.
Hematuria, presence of casts, proteinuria : GN
2.
Proteinuria : Nephrontic syndrome
3.
WBC, bacteria : UTI
4.
Biopsy는 intrinsic renal dz의 확진검사
Ⅲ. Treatment
5.
Prerenal
(1) Dehydration 시 10~20ml/kg crystalloid
(2) hemorrhagic shock 시 수혈
6.
Renal
(1) Fluid overload 시 fluid restriction
(2) Diuretics 사용
(3) Nephrotoxic medication 중단
7.
Postrenal
(1) Fluid restriction, obstruction 시 foley catheter insertion
(2) 아이들에게 oligoanuric AKI 시 hypokalemia나 hypophosphatemia가 증상을 발생시키지 않는
이상, potassium이나 phosphate를 투여하지 말아야 한다.
(3) Diuretics로 fluid overload가 해결되지 않거나 metabolic acdisosis가 bicarbonate로 호전 없을 시
RRT를 고려.
Ⅳ. Nephrotic syndrome
1.
Glomerular capillary wall의 투과도 변화로 단백질 소실 유발
2.
특징 : 단백뇨, 저알부민혈증, 고지질혈증, 부종
3.
진단 criteria
(1) Edema
(2) Proteinuria : 아침 첫소변 Uprotein/Ucr>2 또는 24시간 Uprotein>50mg/kg or 40mg/m2
(3) Hypoalbuminemia : Serum albumin<25gm/L
4.
치료
•
ED에서는 급성 증상 조절에 초점을 맞춘다.
(1) Hypovolemic shock이면 부종 심해도 isotonic fluid로 치료
(2) Volume overload면 furosemide 1~2mg/kg로 치료
(3) Hypoalbuminemia 동반되어 있으면 albumin 0.5~1g/kg 함께 준다.
(4) Nephrotic syndrome의 specific treatment는 oral corticosteroid (2mg/kg/d or 60mg/m2/d),
second line treatment로는 cyclosporine, cyclophosphamide, MMF 등이 있음.
Ⅴ. Glumerulonephritis
1.
Immune complex가 glomerula에 침착하여 발생하는 inflammation process
2.
특징 : hematuria, proteinuria
3.
Ex. : SLE nephritis, GBM, Alport’s sd, PSGN, IgA nephritis, HSP
4.
증상 : 혈뇨(m/c), 고혈압, 두통, 거품뇨
5.
PSGN
(1) group A β-hemolytic streptococci infection
(2) Pharynx(7~14일)나 skin infection(3~5주) 후 hematuria, proteinuria, HTN, edema
(3) ASO↑, anti-DNAse B titer↑, C3↓
(4) 치료 : supportive care
1.
IgA nephropathy
(1) m/c GN, autoimmune dz
(2) 셋 중 1가지로 발현
① Macroscopic hematuria
② Microscopic hematuria + proteinuria
③ Acute PRGN with edema, HTN, renal insufficiency
(3) 치료 : Symptomatic, 면역억제 치료 (경우에 따라)
2.
HSP
(1) 증상 : 자간, 관절통, 복통, 신질환 (Tetrad)
(2) Renal complicataion : 20~54%, 28일내 발생
(3) 치료
① Hydration, pain control
② Steroid는 severe abdominal pain에 도움이 될 수 있으나, renal involve를 막아주지 못해
추천되지 않는다.
3.
HUS (★)
(1) AKI, thrombocytopenia, microangiopathic hemolytic anemia가 생기는 병
(2) 90%에서 shiga toxin-producing E.coli (E.coli O157:H7)가 유발
(3) 덜 익힌 고기, 우유, 과일, 채소
(4) Shiga toxin이 소장을 통해 흡수
→ Microangiopathic intravascular thrombosis, RBC hemolysis, thrombocytopenia
→ Glomerular perfusion↓ → 고혈압, oliguria, anuria
(5) 증상
① E.coli enteritis (구역, 구토, 혈성 설사) ② 빈혈
③ 소변량 감소 ④ 경련
⑤ Encephalopathy ⑥ 고혈압
⑦ 심부전 ⑧ 장중첩
(6) Lab.
① CBC & PBS가 중요 ② MAHA (Hb 5~9)
③ Plt<150K ④ Coombs test negative
⑤ Na+↓, K+↑ ⑥ 대사성 산증
⑦ Bilirubin↑(d/t hemolysis)
(7) 치료
① Supportive care
② Fluid overload만 없다면 early aggressive volume expansion이 도움이 될 수도 있음.
전해질이상 교정, hypovolemia 교정 (수액 10~20 mL/kg N/S)
③ 항생제는 HUS이 위험성을 증가시키기 때문에 소아 설사 환자에서 금기
④ Antiperistalic agent는 E.coli 감염에서 전신 합병증 유발위험있어 금기.
심한 빈혈에는 수혈 필요
PLT 수혈은 thrombotic process 악화 우려로 추천되지 않음
Eculizumab 또는 plasma change가 도움이 될 수 있음.
모든 HUS 환자는 입원이 필요
neurologic Sx.이나 Oliguric renal fialure 환자는 ICU 입원 필요
급성 HUS환아의 50% 정도는 RRT가 필요
95%정도의 환자는 acute phage에서 생존, 대부분 renal function을 회복한다.
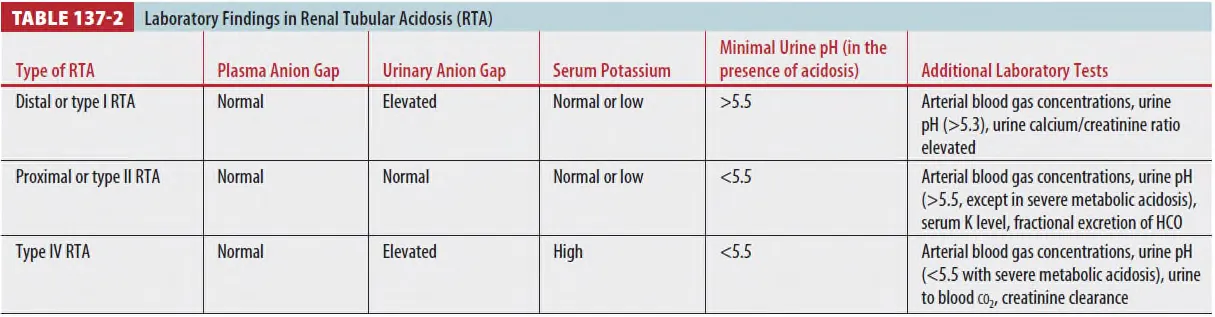
Ⅵ. Renal tubular acidosis
Ⅶ. Hypertension
1.
Hypertensive urgency : BP↑ + End organ damage (-) → 경구 혈압약
2.
Hypertensive emergency : BP↑(99‰ 이상) + End organ damage (+)
→ IV로 첫 8시간 동안 25% 이하 혈압강하
3.
Essential hypertension : 소아보다 청소년기, 신장, 내분비 질환으로 인한 이차성이 많다.
Ⅷ. Hematuria
1.
RBC 5개 이상
2.
Macro hematuria / transient / microscopic hematuria
3.
결석, 최근 감기 앓은 병력
4.
혈압 높거나 단백뇨 동반 시 w/u 필요
