

Ⅰ. 식도 응급
1.
Dysphagia, odynophagia, and foreign body sensation immediately implicate the esophagus.
2.
Symptom : Chest pain, upper GI bleeding, malignancy and mediastinitis
3.
Esophageal foreign body and esophageal perforation : emergency
Ⅱ. Dysphagia
4.
‘Difficulty with swallowing’
5.
Oropharyngeal dysphagia (Transfer Dysphagia)
(1) 삼킴 초기에 삼키기 시작의 어려움.
(2) 음식물이 구강인두에서 상부식도 괄약근으로 이동할때
6.
Esophageal dysphagia (Transport Dysphagia)
(1) 음식물이 식도 아래로 이동하거나 lower sphincter를 통과하는데 장애
7.
Cause
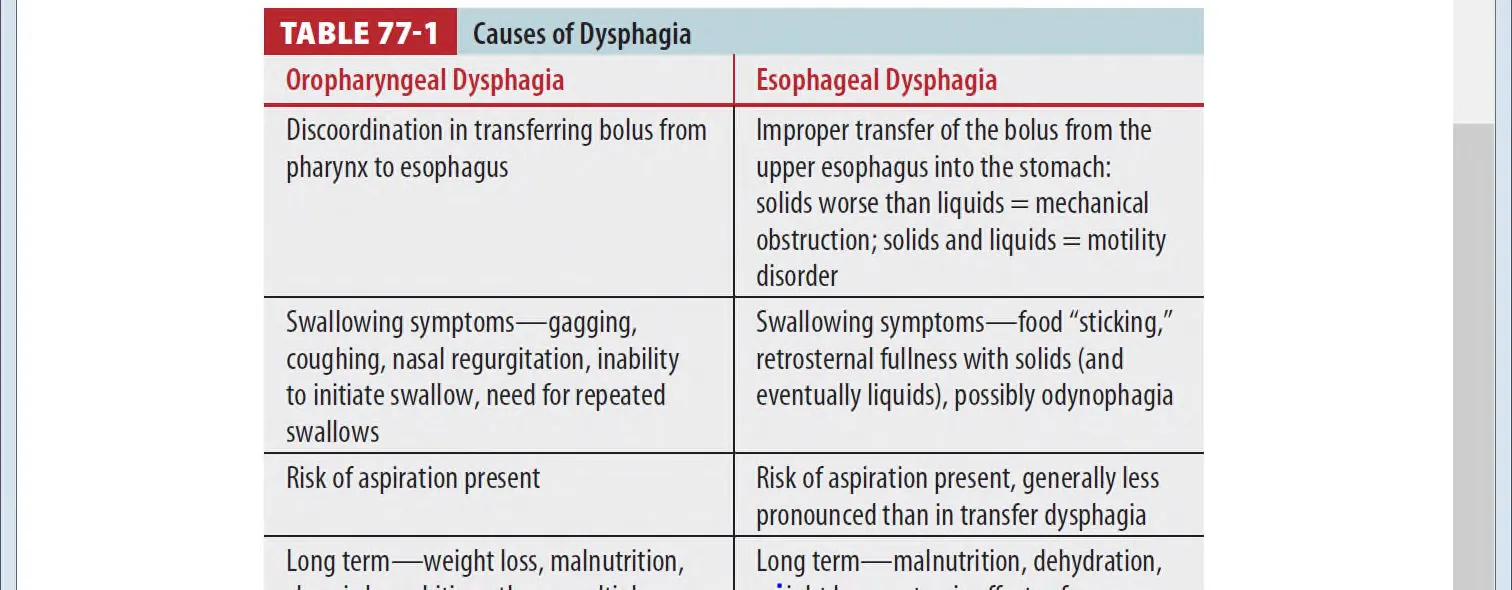
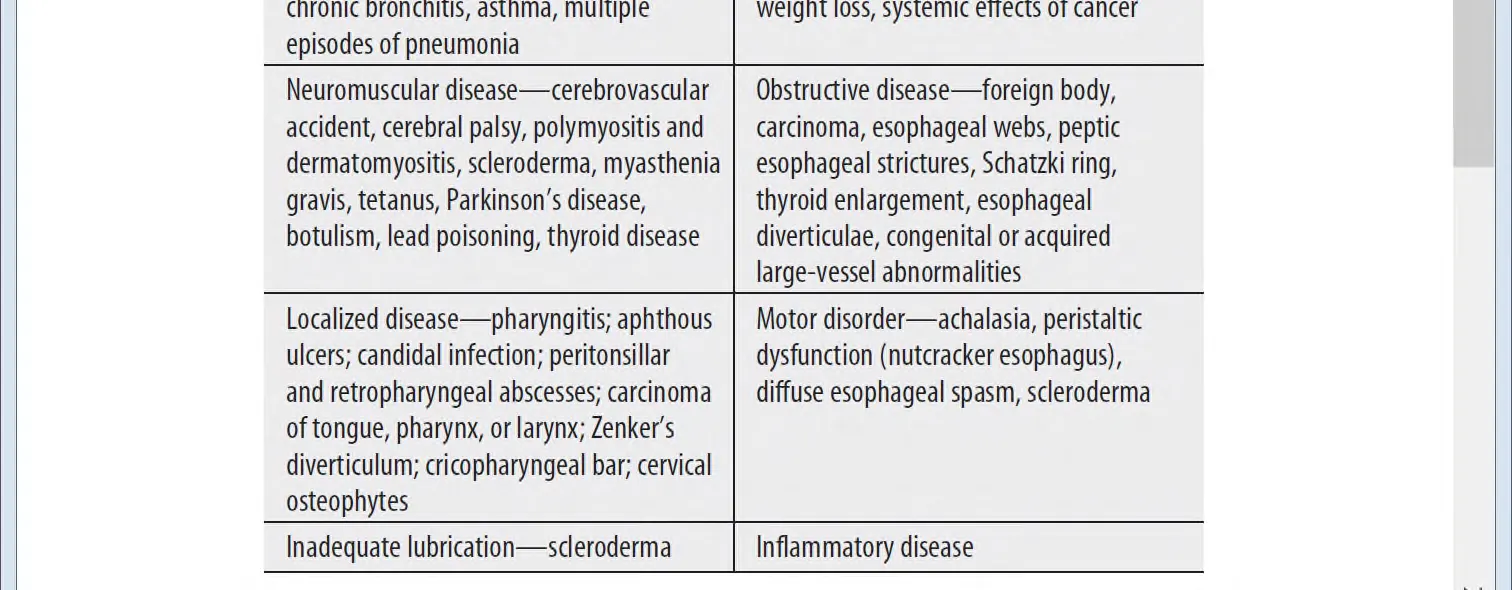
5.
Symptom
(1) Throat and chest pain with swallowing 동반
(2) Mechanical or obstructive disease는 점점 악화, 처음에는 고체 이후 액체 삼키기 힘듬
6.
Diagnosis
(1) Upper endoscopy, videoesophagography, barium swallow, or esophageal manometry
(2) History나 신체검진에서 malignancy 의심 시, CT imaging of neck and chest may be
indicated in the ED
Ⅲ. GERD
1.
Cause

2.
증상
(1) Heartburn
(2) Chest discomfort
① Cardiac origin과 양상이 비슷한 경우 있음
② 히스토리 및 악화 완화 요인 등을 파악해야 함
(3) Odynophagia
(4) Dysphagia
(5) Acid regurgitation
(6) Discomfort with meals, and hypersalivation
(7) 고개 숙이거나 압이 올라가는 상황에서 악화
3.
GERD complication
(1) Strictures (2) Dysphagia (3) Inflammatory esophagitis
(4) Barrett’s esophagus (5) Asthma exacerbations (6) Sore throat
4.
치료
(1) 위에서 산분비 억제
(2) Upper track에서 motility 강화
(3) Risk factor 제거
(4) 적절한 치료는 is unclear
① 처음 치료의 시작은 with histamine-2 receptor antagonists
② 2주 후에도 효과가 없다면 start a proton pump inhibitor
(5) ED 퇴원 시 GERD 악화시키는 물질 피하기(ethanol, caffeine, nicotine, chocolate, fatty foods),
수면 시 head up (30 degrees), 수면 3시간 전 음식섭취 피하기
Ⅳ. Esophagitis
•
내시경 검사에 의해 진단 확립
1.
Inflammatory esophagitis
(1) GERD가 lower esophageal mucosa에 inflammatory response를 유발
→ 시간이 지나면서 esophageal ulceration, scarring, stricture로 발전
(2) Treatment
① 약물치료로 acid-suppressive medications
② 유발물질 피하기
(NSAIDs and other anti-inflammatory drugs, potassium chloride, and some antibiotics )
2.
Eosinophilic esophagitis
(1) Inflammatory response (foods, allergens, or acid reflux)
(2) 진단 : 내시경
(3) Treatment
① 알러지 유발 물질 피하기
② Oral liquid corticosteroids or inhaled corticosteroids
③ Strictures 있다면 dilatation 필요
3.
Infectious esophagitis
(1) 면역억제환자에게서 나타날 수 있으며, candida (m/c), herpes simplex, aphthous ulceration...
(2) Endoscopy with biopsy and specimen culture establishes the specific diagnosis
(3) Candidiasis Empiric treatment : Oral fluconazole, 400 milligrams per day for 2 weeks
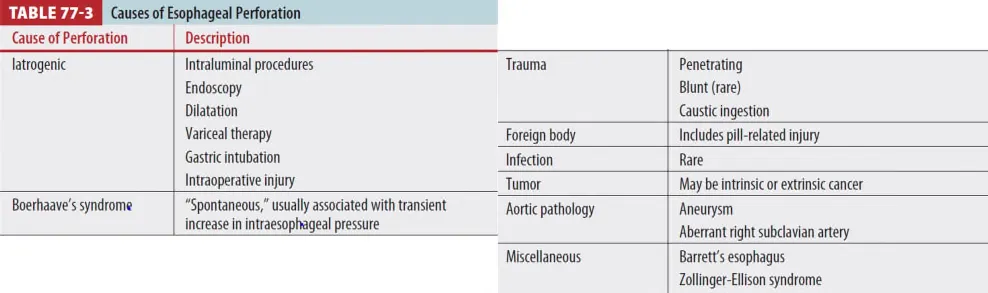
Ⅴ. Esophageal perforation
1.
Cause
2.
Pathophysiology
식도 내용물이 (1) mediastinal, pleural, peritoneal로 유출되면 dramatic한 임상양상을 초래
(2) Fulminant necrotizing mediastinitis, pneumonitis, peritonitis로 급격히 진행 shock 유발.
(3) 흔히 spontaneous perforations은 distal esophagus의 left posterolateral wall에서 발생
(4) Proximal perforation : 기계조작에 의해 잘 일어나며 distal perforation다 less severe
3.
Clinical features
(1) Described as acute, severe, unrelenting and diffuse
(2) Location : Chest, Neck, Abdomen
(3) Radiate to the back and shoulders, or back pain may be the predominant symptom
(4) Exacerbated by swallowing.
(5) Dysphagia, dyspnea, hematemesis, and cyanosis 역시 관찰되기도 한다.
4.
Physical examination
(1) Abdominal rigidity with hypotension, fever → often occur early
(2) Tachycardia, tachypnea : common
(3) Cervical esophageal perforations → Cervical subcutaneous emphysema
(4) Mediastinal emphysema
(5) "Hamman’s crunch" - 청진 (by air in mediastinum)
(6) Pleural effusion가 pleural space로 유출시에 동반되기도
5.
Diagnosis
(1) IV contrast CT : neck or chest
(2) CT 상 이지 않지만 임상적으로 가능성이 높으면
→ Flexible video esophagoscopy or esophagography
(식도 내시경 : Sensitivity 95~100%, Specificity 90~100%)
(3) 숙련된 내시경 의사가 없는 경우에는 esophagography with water soluble contrast material
(ex. gastrografin)
6.
Treatment
(1) 진단 즉시 수술 고려
(2) Shock 상태 환자는 적절한 resuscitate
(3) Broad spectrum parenteral antibiotics
Ⅵ Swallowed Foreign bodies and food impaction
1.
Pathophysiology
(1) 18~48개월 소아나 의식장애가 있는 환자에게 주로 FB ingestion이 발생.
(2) Pylous를 통과하면 GI tract에 문제를 일으키는 경우는 드물지만, 모양이 irrgeular or sharp 하거나
2.5cm 이상 넓거나 6cm 이상 길면 pylorus distal에 걸릴 수 있음.
(3) Esophageal impaction은 airway obstruction, stricture, perforation를 일으킬 수 있음.
2.
Clinical Features
(1) 성인
① 명확한 history, retrosternal pain과 물체 위치를 localizing 함
② Dysphagia, vomiting, choking 있을 수도 있음
(2) 소아
① 불명확한 history, 식이 거부 및 불가, 구토
② Choking, gagging, stridor, neck or throat pain, drooling의 증상 관찰
③ 2세 미만의 소아는 특히 눈에 띄지 않는 섭취에 대해서 의심이 필요
3.
진단
(1) Plain X-ray,
(2) CT scan (high-yield test, perforation and subsequent infection 등에 탁월)
4.
치료
(1) Endoscopy
① Airway compromise에 임박한 환자는 resuscitated 및 Airway management가 필요
② Esophagus의 완전한 막힘(distal esophageal food impactions)은 secretions과 aspiration 등
근위부의 pooling을 제공하기도 함.

(2) Laryngoscopy
① Stable한 환자, 초근위부 물질 제거 위해 laryngoscope, fiberoptic scope 시도할 수 있음
(3) Expectant Treatment (대기요법)
① Benign한 모양이거나 자연스러운 모양이 pylous distal에 있으며, 환자가 편안하고 입으로 섭취 가능
시 기대해 볼 수 있음
(4) Distal GI tract 이물은 수술 consult 필요할 수 있다.
(5) Foley catheter removal
① 일부 저자는 alternatives to endoscopy
② Blunt foreign body 24hr 이내
③ Underlying esophageal disease가 없는 자
(6) Glucagon
① Distal esophagus object에서 성인 1 to 2mg IV
② 성공률은 낮다.
Ⅶ. Special Considerations
1.
Food impaction
(1) 고기가 가장 흔한 원인
(2) Complete esophageal obstruction 이나 뼈조각을 포함한 food impaction인 경우 응급 내시경이
필요하다.
(3) Uncomplicated food impaction은 expectantly하게 치료.
(4) 시간과 진정이 도움 그러나 덩이가 12~24시간 동안 막힌 채 허용해서는 안 된다.
(5) Proteolytic enzyme (Eg, Adoph’s Meat Tenderizer, contains papain)는 금기
→ Severe mucosal damage, esophageal perforation을 유발할 수 있다.
(6) Glucagon therapy를 사용한다 (Initial 1~2mg IV, 20분 후 통과 안되면 1번 더 사용 가능)
2.
Coin ingestion
(1) Endoscopy 사용 : 아이들에게서는 esophageal coin 제거를 위해 endoscopy 사용.
(2) Foley catheter로 제거는 fluoroscopy 하 시행
① 흡인을 막기 위해 Trendelenburg position
② Advanced airway manage 가능해야 한다.
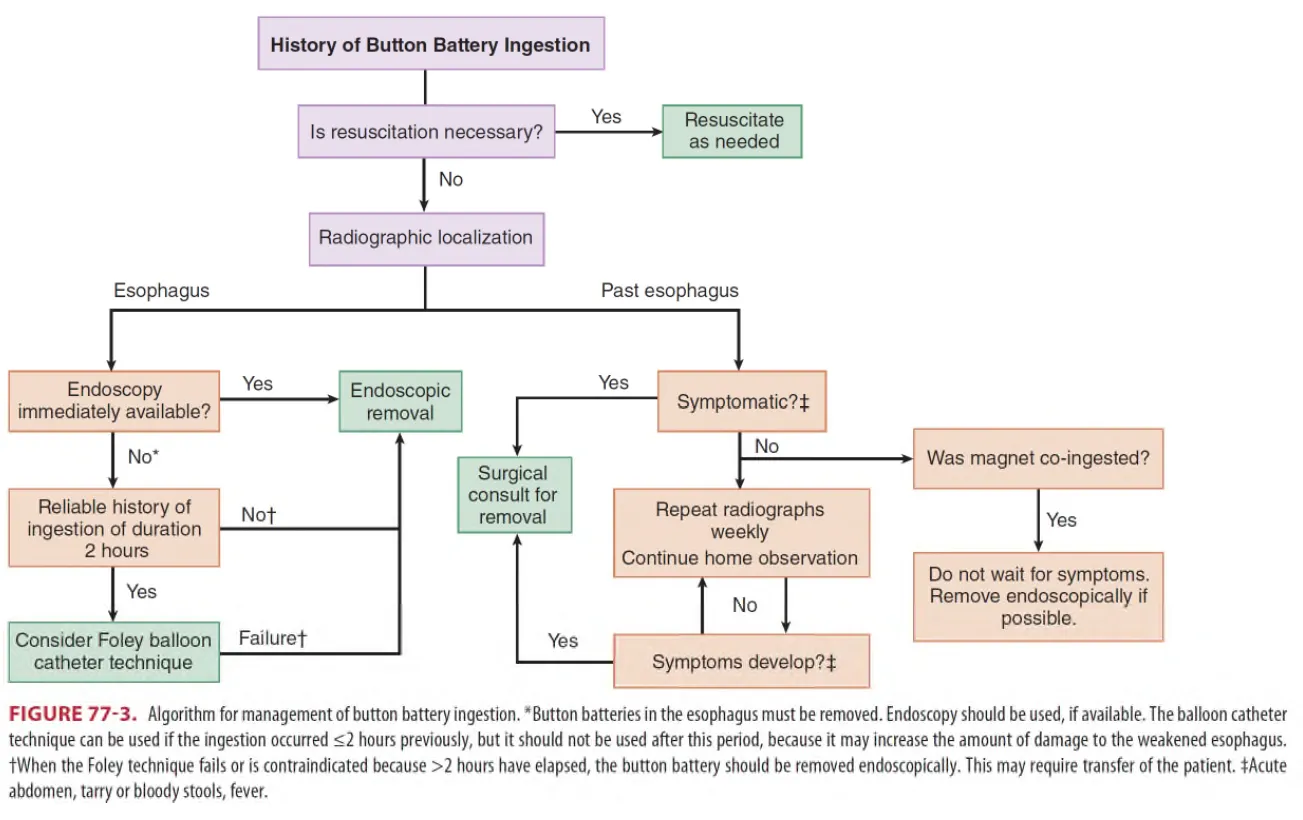
3.
Button battery ingestion
•
True emergency
•
식도에 걸리면 mucosal injury, necrosis 유발, 6시간 내 perforation 발생 가능
(1) 식도에 있을 때
① 내시경 이용 가능 - 내시경적 제거
② 내시경 이용 안되면
: 2시간 이내 섭취한 신뢰할 만한 History → Foley ballon catheter 고려
: 2시간 이후 또는 Foley 실패 시 → 내시경적 제거
(2) 식도 통과 시
① 증상 없으면 X-ray 반 촬영 및 경과관찰
—> 대부분의 battery는 48~72 시간 내에 몸을 빠져 나온다. (길게는 14일이 걸린 경우도 있음.)
→ 48시간 내에 pylorus 통과 못하면 제거
② GI tract injury 증상이 있으면 즉시 surgical consult for removal
4.
Ingestion of Sharp objects
(1) 즉시 제거해야 한다.
(2) 위의 원위부를 통과한 날카로운 물체로부터 장 천공은 흔하기 때문에, American Society for GI
Endoscopy guidelines에서는 날카로운 물체가 위나 십이지장에 있는 동안 내시경으로 제거를 권고한다.
(3) 장천공이 일어난다면 통 IC valve에 있음.
(4) 증상이 없고 십이지장의 원위부에 물체가 있다면 daily plain X-ray 로 passage를 확인
(5) 3일이 지나도 빠져나오지 않으면 수술적 제거를 고려
(6) Intestinal injury (pain, emesis, fever, GI bleeding)의 증상이나 sign이 있으면 즉시 surgical
consult
5.
Narcotics ingestion
(1) 일반 필름으로 관찰 가능
(2) Endoscopy는 Iatrogenic perforation 위험성으로 금기
(3) 패킷이 intact하게 잘 통과할 것 같으면 직장에 도달할 때까지 관찰.
