01837600 구모경 용혈성 빈혈, r/o TTP 사례
A. Introduction
•
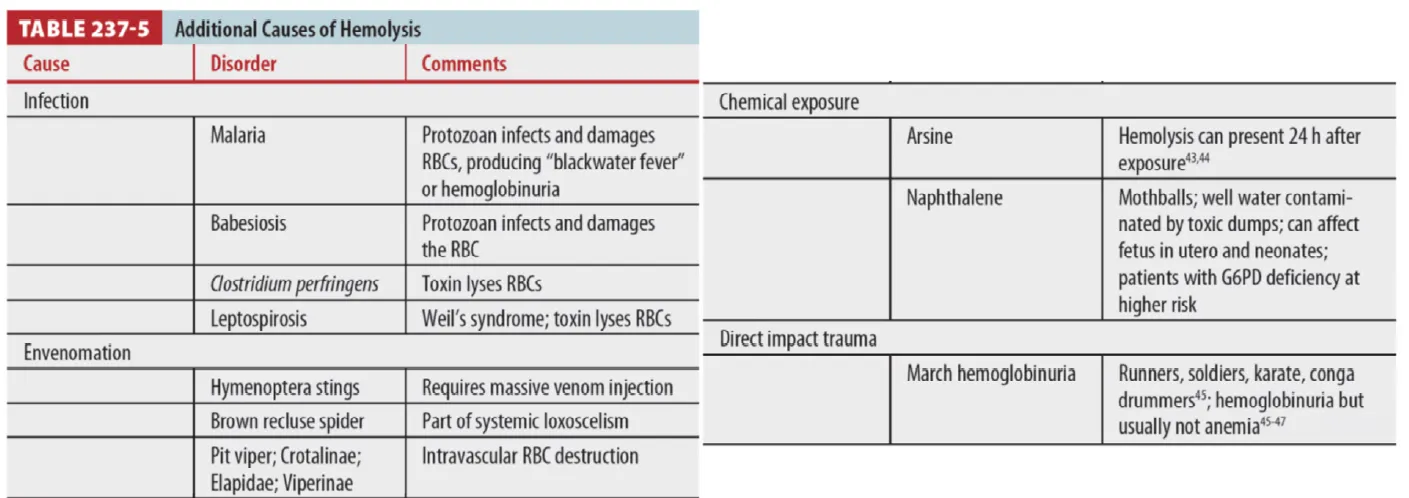
Hb 생성 또는 RBC 막의 유전적/선천적인 질병 떄문이 아닌 RBC의 파괴가 특징
•
혈관 내 or 혈관 외 (Extravascular, 주로 비장과 간)에서 용혈이 발생.
•
RBC 파괴 → Free Hb → Bilirubin으로 분해 → conjugated bilirubin
•
Conjugated bilirubin은 배출되나, 간의 대사 능력을 넘은 비결합 빌리루빈은 Jaundice, Darkened urine 일으킨다.
(1) 증상
•
asymptomatic ~ severe hemodynamic compromise까지 있다.
•
Weakness, Fatigue, Dizziness, Shortness of breath, DOE, Tachycardia, Palpitation, Chest pain,
New/Accentuated cardiac murmur, Pallor
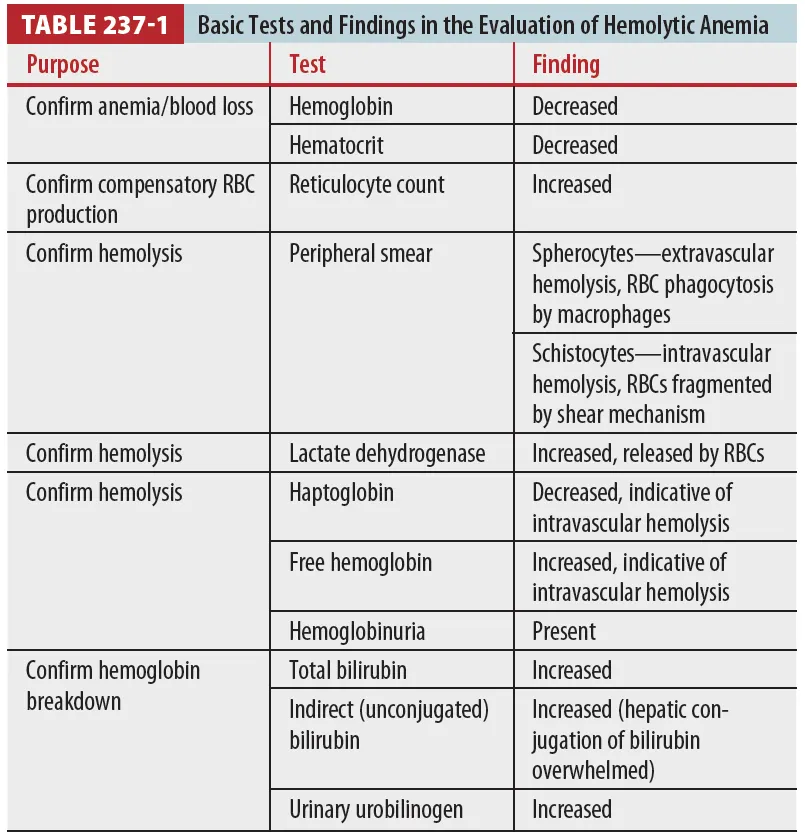
(2) Lab finding
•
RBC hemolysis, Hb breakdown, Compensatory RBC production
B. Immune mediated acquired hemolytic anemia
•
Autoimmune, Alloimmune, Drug-induced
B1. Autoimmune hemolytic anemia
•
자신의 RBC에 대한 Antibody 생성
•
진단 : Coombs test (RBC에 대한 Ab 규명)
•
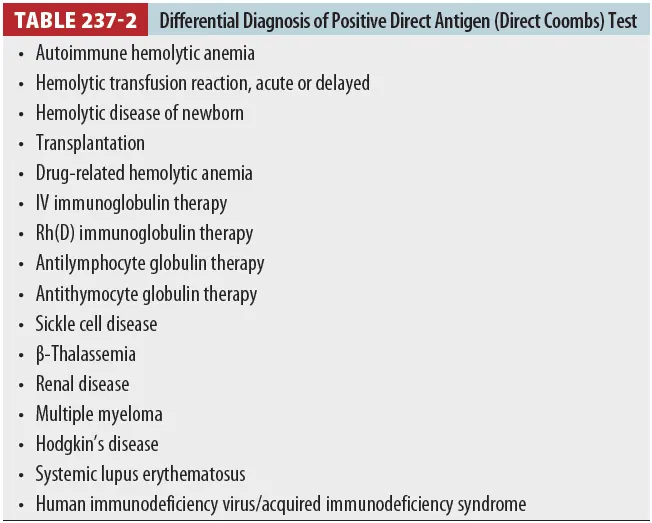
Direct Coombs test (= Direct antigen test)
◦
RBC surface의 IgG or complement 확인
◦
Specific하지 않고 (Table237-2), severity 확인 불가
Indirect Coombs test - Specific surface autoantibody를 찾는다.
•
Primary vs secondary disease
: Primary(idiopathic) 는 원인미상
: Secondary disease 는 underlying disorder와 연관
: 대부분에서 초기에는 primary로 진단되나 이후 lymphoproliferative, autoimmune, or infectious
diseases와 연관 확인됨.
: AIHA의 autoantibody type별 category - warm, cold, mixed type (Table 237-3)
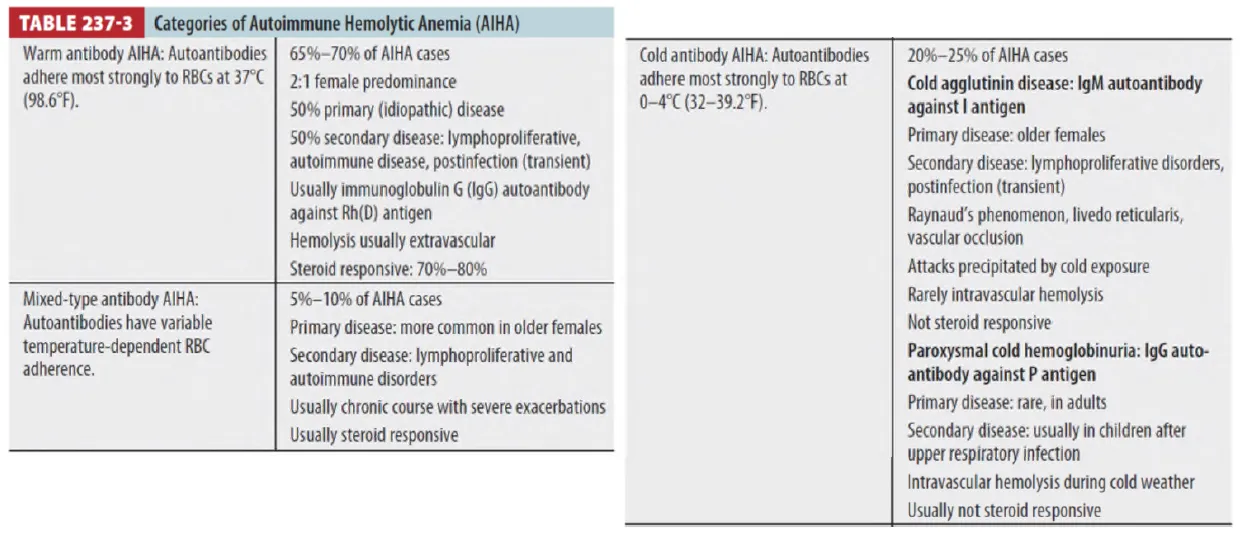
(1) Warm antibody autoimmune hemolytic anemia
① 대부분 Extravascular hemolysis
② Treatment
: Initial High-dose steroids - Oral prednisone, 1~1.5mg/kg/day, 3~4 weeks
: Monoclonal Abs (e.g., Rituximab) or Immunosuppressants
: Splenectomy
•
제거 후 감염과 패혈증에 취약
•
무서운 합병증인 overwhelming postsplenectomy infection 예방 위해 Pneumococcal,
Menigococcal vaccinine과 Penicillin daily 복용(첫 수년)
: Severe hemolysis - Plasma exchange (Steroid, 면역억제치료 효과 기다리는 동안)
: Life threatening anemia에서 Allogenic RBC 수혈
→ Antigen 반응 검사를 해야 하지만 매우 힘들고 시간도 오래 걸리므로 응급 상황에서는 Close
monitoring 하면서 필요로 하는 최소양만 천천히 수혈함
(2) Cold antibody autoimmune hemolytic anemia
① 낮은 온도에서 Peripheral smear시 RBC의 응집
② RBC 표면의 Complement fixation과 관련 (Complement cascade)
③ Hemolysis는 Extra/Intravascular space 모두에서 일어남
④ Extravascular RBC 파괴는 Hepatic macrophage(Kupffer cell)이 대부분 담당
⑤ 주요 질환 : Cold agglutinin disease, Paroxysmal cold hemoglobinuria
(3) Mixed type autoimmune hemolytic anemia
① RBC에 대한 Warm, Cold autoAb 혼재
② 대게 Lymphoproliferative, Autoimmune disease와 관련됨 (특히 SLE)
③ 치료 : Steroid, Splenectomy, Immunosuppressant
B2. Alloimmune hemolytic anemia
(1) Allogenic RBC 노출 후에 AlloAb 생성됨
(2) AlloAb는 Allogenic RBC에 반응하며 환자의 RBC에는 반응하지 않음
(3) Hemolytic disease of the newborn
: Rh (D) negative meternal immune system이 Rh (D) positive fetal RBC에 노출되면 IgG
AlloAb를 생성
→ AlloAb는 태반을 건너가 Fetal RBC destruction하며 증상 유발 (mild ~ fetal death)
(4) Anti-D IgG : Fetomaternal hemorrhage의 상황이나 출산 직후에 투여하면 Maternal AlloAb
생성 억제하여 hemolytic disease of the newborn을 예방
(5) 치료 : Intrauterine and intravascular fetal transfusion, plasma exchange, IVIG
(6) 대부분은 RBC 수혈 과거력이 있으며 다음 수혈 시 즉각적으로 fever, chest and flank pain,
tachypnea, tachycardia, hypotension, hemoglobinuria, and oliguria가 생긴다.
(7) 3~7일 후에 증상이 생길 수 있다.
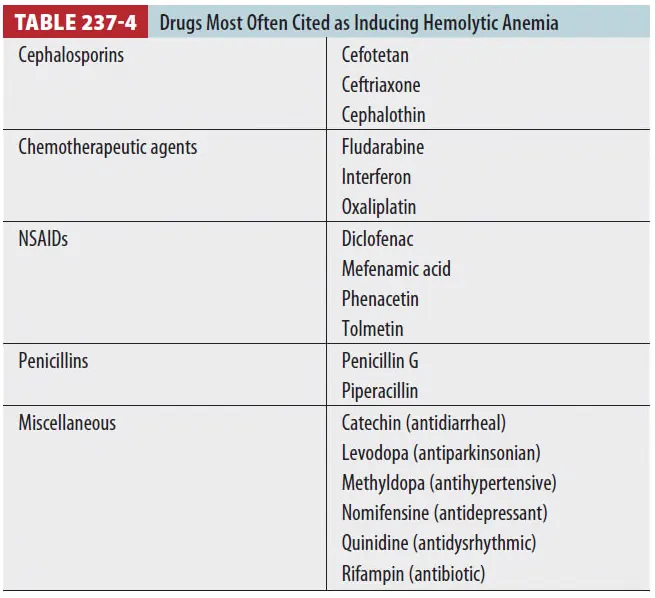
B3. Drug-induced hemolytic anemia
(1) 드물며 AIHA와 간별 어렵다.
(2) 치료 : 약물 중단, 수혈, Severe한 경우 Steroid
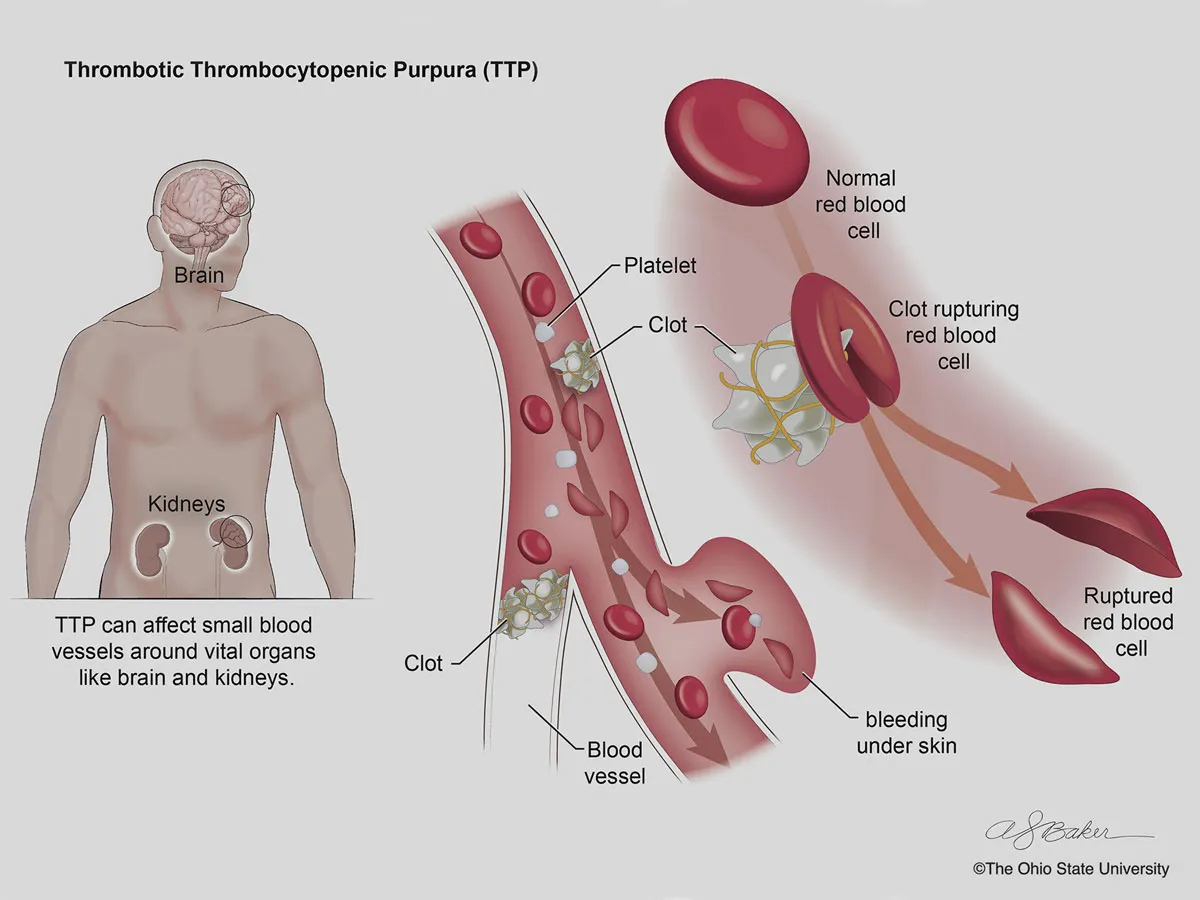
C. Microangiopathic syndromes
•
2개의 Classic syndromes
Thrombotic thrombocytopenia purpura (TTP) : 주로 성인, 신경학적 문제
Hemolytic uremic syndrome (HUS) : 주로 소아, 신장에 문제
•
두 질환 모두 Microvascular circulation 내에 vWF를 매개로 한 PLT 응집과 관련있음.
부분적으로 폐쇄된 Arteriole, Capillaries을 지나며 RBC가 fragmentation되어 발생.
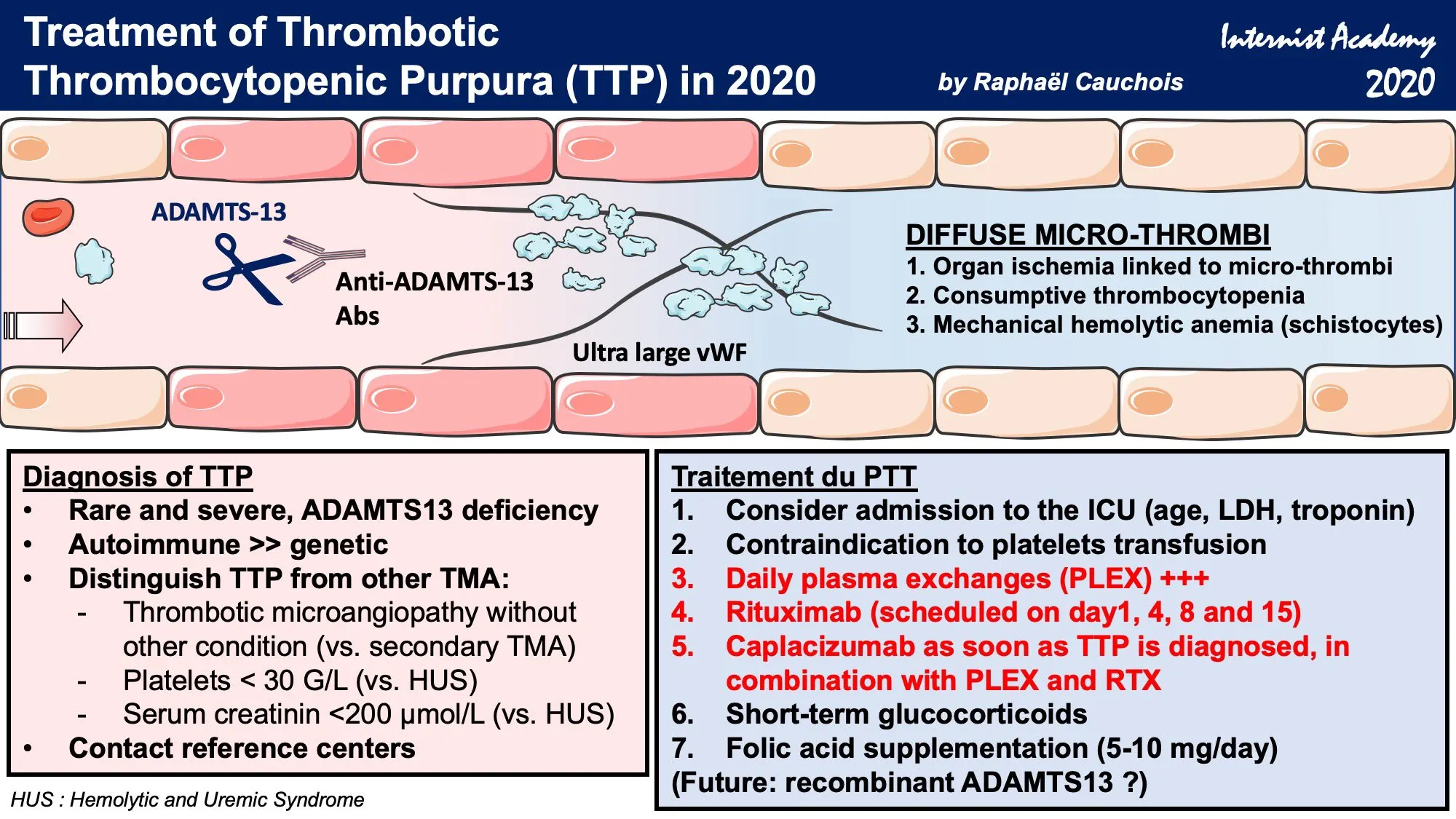
C1. Thrombotic thrombocytopenia purpura (TTP)
•
치료하지 않으면 High mortality
•
Plasma exchange 후 80% 이상에서 Remission 기대 가능
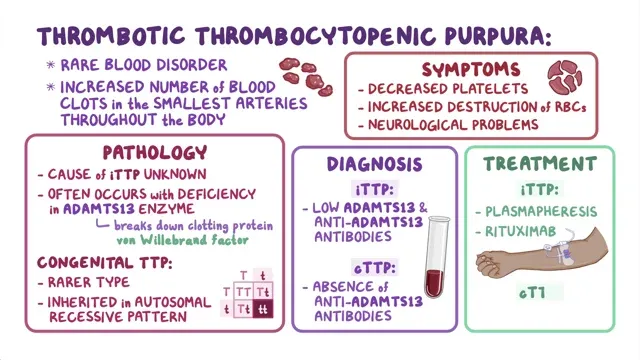
(1) Sx. Pentad
•
CNS abnormalities
•
Renal pathology
•
Fever
•
Microangiopathic hemolytic anemia
•
Thrombocytopenia
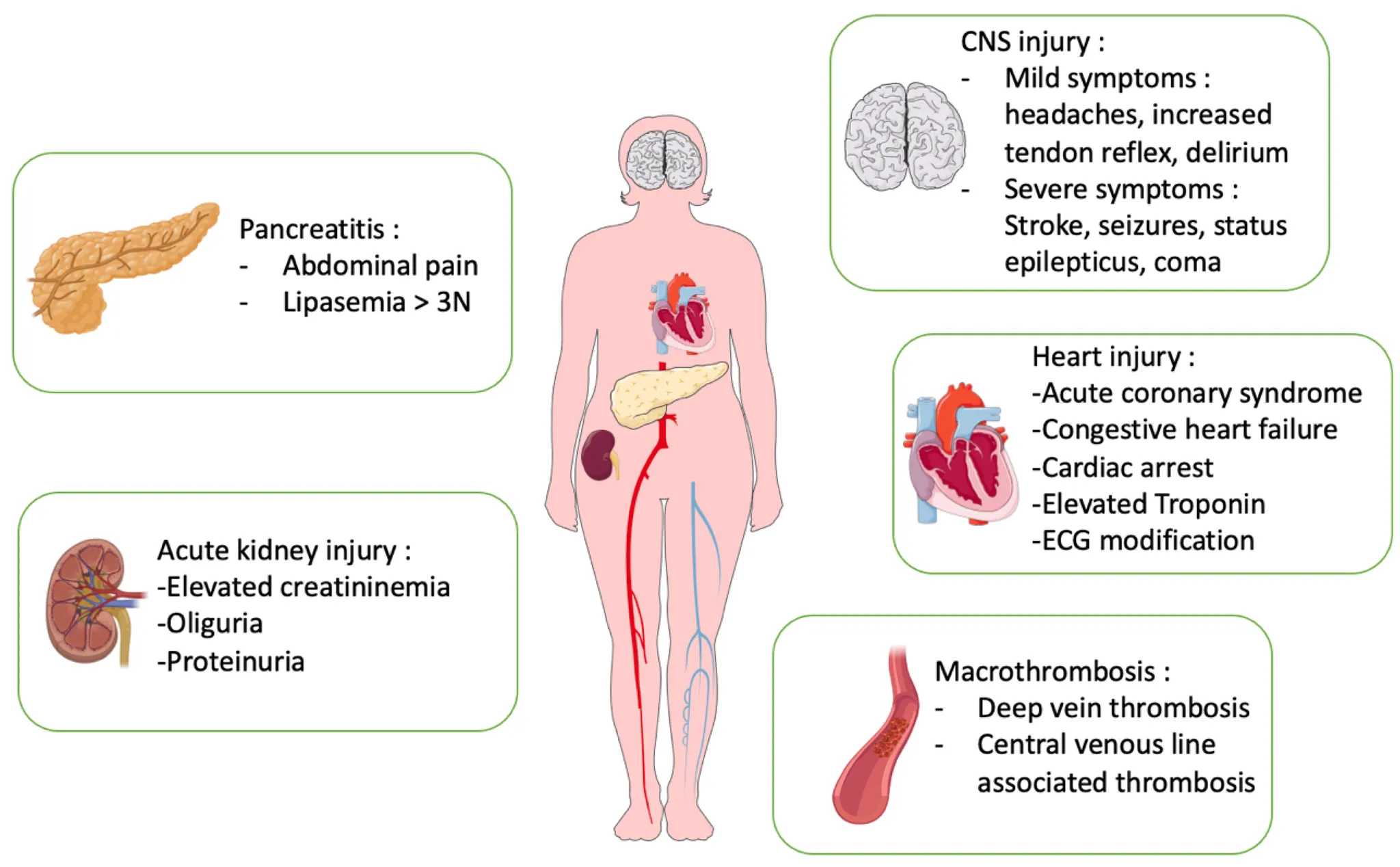
(2) Clinical features
•
Microthrombi가 RBC를 깨며 Microangiopathic hemolytic anemia 발생
•
TTP에 의한 PLT aggregation에 의해 Thrombocytopenia 유발됨
•
Microthrombi가 CNS/Renal의 Arteriole, Capillaries에 쌓이면 Seizure, Stroke, Other focal
neurologic deficits, Coma, Acute renal injury 발생
•
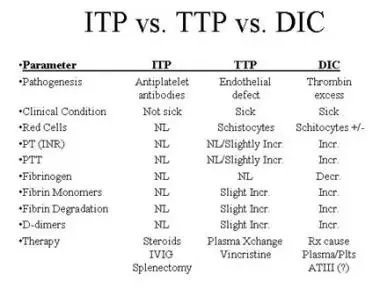
TTP thrombi는 Fibrin이 포함 되지 않기 때문에 정상 Coagulation 보여, DIC와 구별된다.
•
임상 양상과 lab 결과가 preeclampsia–eclampsia, HELLP syndrome (hemolysis, elevated liver
enzymes, low platelet count), and acute fatty liver of pregnancy와 비슷하다.
: Preeclampsia/HELLP syndrome 증상이 심한 24주 미만 임산부에서 TTP를 의심
(3) Treatment
•
Plasma exchange (구리병원에서는 어렵다)
: 효과적, Daily plasmapheresis of 40mL/kg or 환자 Plasma volume의 1.0~1.5배까지
: 2~3일 연속 정상 PLT count 도달할 때까지 한다
•
Plasmapheresis가 즉시 시행되기 어려우면 FFP infusion 먼저 시작
•
Plasma allergy 있는 사람에게는 Specialists와 상의 하에 Ⅷ concentrate (Containing ADMTS 13 activity)를 Infusion 해 볼 수 있음
•
Severe TTP의 경우 RBC transfusion, Anticonvulsants, Antihypertensives, Hemodialysis와 같은
처치가 필요할 수도 있음
•
Life threatening bleeding이나 두개내 출혈을 제외하고 PLT 수혈은 피해야 함
(Thrombosis 악화되어 renal failure 나 사망에 이를 수도 있음)
•
Aspirin은 Severe thrombocytopenia 상태에서 출혈성 합병증을 악화시킬 수 있으나 PLT 수가
적절하다면 Cerebrovascular, Cardiovascular indication 시 사용
•
Heparin은 not beneficial
•
Autoimmune TTP:Corticosteroids, Rituximab, Cyclosporine
•
Drug-associated TTP에서는 약물 중단
(4) 유발/악화 인자
: pregnancy, infection, inflammation, medcation use
C2. Hemolytic uremic syndrome (HUS)
(1) 소아 AKI에 흔한 원인
(2) Microangiopathic hemolytic anemia, Thrombocytopenia, Acute nephropathy
(3) Typical vs Atypical
① Typical (90%)
: 소아 (1~4세), 감염성 설사 1주일 내 발생,
: 원인 - 주로 E. coli (O157:H7), 외 Shigella, Yersinia, Campylobacter, Salmonella
② Atypical
: 4세 이상 소아, 성인, Extrarenal. TTP와 감별 어려움,
: 원인 - S. pneumoniae, EBV, BM 이식, Immunosuppressant, 항암제 등과 관련
(4) Clinical features
① 설사 후 2~14일에 발생, 복통(+) 혈변(+ or -). 열은 대게 없음
② Nonbloody diarrhea 환자 : Stool 검사로 Occult inflammatory colitis 확인
→ Stool culture에서 E. coli 0157:H7 확인
③ Bloody diarrhea 환자 : Shiga toxin producing bacteria 동정하고 지역전파 예방.
(5) Treatment
① Supportive : Hydration, anemia 심하면 수혈 Anemia, RF 시 투석
② E. coli 0157:H7 감염
: Antimotility drug 금기 → HUS 악화
: 항생제는 Controversial (Shiga toxin 발현이 증가, HUS 진행)
③ Atypical HUS에서는 Eculizumab
(6) Outcome
① Typical HUS : 55~70% AKI 발생, 85%에서 신기능 회복, 5~15% 사망
② Atypical HUS : 50%에서 영구적 신부전, 신경학적 손상 발생, 25% 사망
Aggressive Tx. (Eculizumab) 예후를 좋게 함
D. Macrovascular hemolytics
1.
Prosthetic heart valves 환자에서 발생
2.
구형에서 valve deteriorate 되어 hemolysis, 신형에서 paravalvular leak
3.
특히 Mitral valve replace 후 심각한 증상을 유발할 수 있음
4.
Intracardiac patch repair, Aortofemoral bypass 후나 Coarctation of aorta, Severe aortic valve
dz, Ventricular assist devices있는 환자에서도 발생.
5.
Extracorporeal circulation을 이용하는 환자
6.
치료
(1) Hemolysis에서 Reticulocytosis 위해서 Iron, Folate 처방
(2) Beta blocker : HR 감소되면 RBC shear stress를 줄인다.
(3) Pentoxifylline (Xanthine derivative)
: 혈액의 Viscosity를 줄이고 RBC flexibility, Deformability를 향상시킴
→ 인공판막에 의한 Hemolysis 감소