
A. Pharmacology
: 모든 opioid는 μ-receptor activity를 가진다. → 진통, 진해, 축동, 기분고조, 호흡저하
B. Pharmacokenetics
B1. Opioid는 경구 복용 30분~60분 내 혈중최고농도에 달한다.
1.
대부분의 opioid는 first-pass hepatic metabolism을 거친다.
→ 경구보다는 정맥주사 시 더 효과가 크다.
C. Clinical features
C1. Opioid intoxication toxidrome
(1) Triad : 축동 (miosis), 무기력 (lethargy), 호흡저하 (respiratory depression)
(2) GI Sx : 구역/구토, 장마비
(3) Urinary Sx : 요정체
(4) Local Sx : 두드러기 (IV 주사부위 histamine release effect)
(5) Cardiovasc : 기립성 저혈압
(6) Respiratory : 호흡저하 (얕고 느린 호흡), 기도연축 (bronchospasm)
•
Opioid-induced acute lung injury
: 중증 과다목용 환자에게서 드물게 나타남
: 치료 - 보존적 치료 (기계환기가 필요할 수도 있다)
(7) 그 외 : 저체온, 횡문근융해증 및 신부전, 구획증후군(compartment syndrome)
•
C2. Serotonin syndrome
: 특정 opioid(meperidine, tramadol, dextromethorphan)과 MAOi, SSRI를 같이 복용할 때
이 경우 naloxone은 효과가 없다.
D. Diagnosis
D1. Combination
: Triad (무기력/기면상태, RR <12, miosis) + 의심 정황 (주사자국 등)
D2. Urine screening
(1) 1회 복용 2~4일 뒤에도 positive가 나온다.
(2) False positive 보일 수 있는 다른 약제들이 있다.
E. Treatment
1.
Airway protection & ventilatory maintenance
2.
Decontamination : activated charcoal
3.
Naloxone
•
Competitive antagonist at all opioid receptors
(1) Chronic user : 저용량 (0.04mg IV). opioid withdrawal symptom을 줄일 목적
(2) Naive user : 통상용량(0.4mg IV)
(3) 호흡정지환자 : 고용량(2.0mg IV), 2~3min마다 반복. 최대 10mg
(4) IV infusion : “깨울 수 있던 최소용량(wake-up dose)” 의 2/3를 1시간 동안 투약
(5) IV 확보되지 않을 때 : 2mg을 IM/SC/intranasal/Nebulizer로 공급할 수 있다.
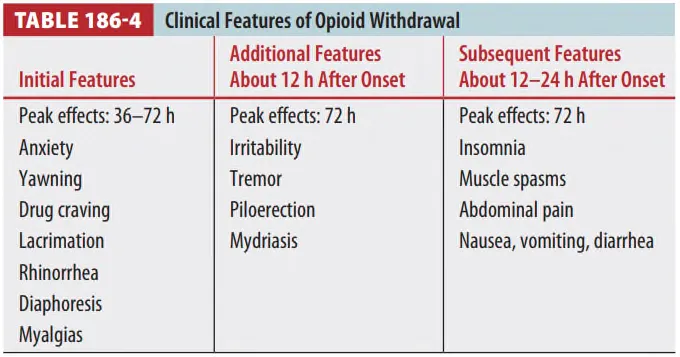
F. Opioid withdrawal
F1. 증상 및 경과
(1) 6~12시간 뒤 불안/하품/drug craving → Tremor, 발기, 근연축, 소화기증상
(2) 3일에 증상이 peak에 이르고 5-6일 째 소실됨.
(3) 거의 life-threatening하거나 fetal 하지 않다
F2. 치료 : 기본적으로 대증치료
(1) Clonidine (α2-agonist) : 중추신경계 증상 완화
(2) Opioid replacement therapy : methadone, buprenorphine
→ Opioid withdrawal이 발생하지 않은 환자에게서 먼저 투약하면 안된다.

