A. Introduction
1.
Wheeizng : High-pitched sound d/t elevation of airway resistance d/t obstructive process
(1) Stridor : Upper airway obstruction (above the thoracic inlet), marked inspiration
(2) Wheezing : Lower airway obstruction (distal to the thoracic inlet), marked expiration
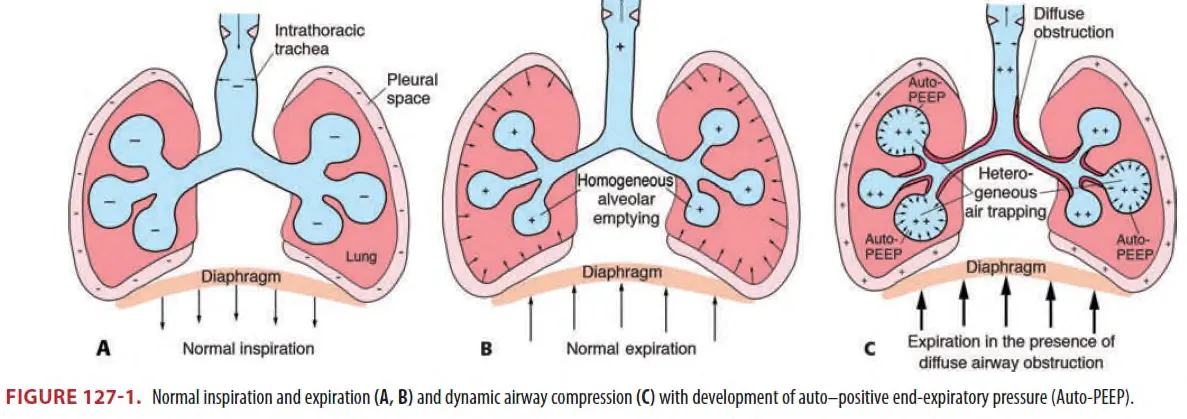
B. Respiratory physiology
•
Diffuse(asthma, bronchiolitis) or focal(foreign body) intrathoracic airway obstruction이
있으면 기도저항을 극복하기 위해 복근 및 intercostal muscle을 사용하게 된다.
⇒ 그러면 Intrapleural pressure의 양압이 걸리고 이것은 기도에 더 저항을 가하게 되어 dynamic airway compression이 발생한다.
⇒ Dynamic aiway compromise는 결국 호기시간을 길게 하여 end expiration 때 alveoli에 air traping을 초래하고 이것은 다음 호흡 cycle에서 auto-peep을 유발하여 VQ mismatch, hypoxemia를 유발한다.
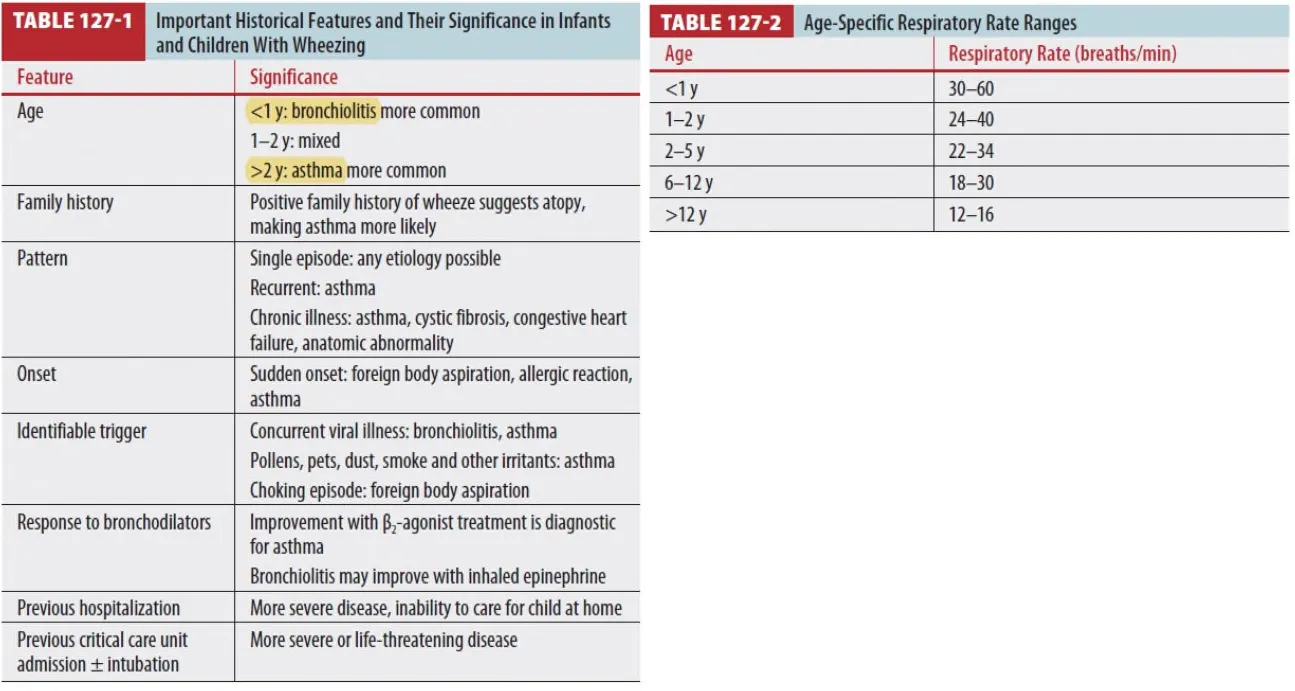
C. Wheezing
•
6세 환아의 약 50%는 wheezing을 경험한다
•
2세 이상 환아 : Recurrent or episodic pattern, trigger와의 연관성, bronchodilator effect가 있는
것은 asthma의 가능성을 크게 시사
•
1세 미만 : Viral season 동안 sick contact, nasal congestion, poor feeding은 bronchiolitis를 시사
C1. Clinical features
(1) P/ex assessment triangle : Appearance, Work of breathing and Circulation
•
General appearance : TICLS (Tone, Interactivity, Consolability, Look, and Speech)
•
Work of Breathing : position(sniffing,tripod), accessory m. use, stridor or wheeze
•
Circulation : cyanosis
•
Respiratory rate : Table 127-2 참조. 꼭 1분 Full로 잴 것.
•
Mild hypoxemia (92-94%)
:Supplemental O2 필요함. <92% 이하의 hypoxemia는 moderate severe disease 시사
•
Diaphoresis, confusion and drowsiness 있으면 imminent respiratory failure!
•
Inspiratory-to-expiratory ratio가 정상인 2:1보다 작으면 (eg., 1:2, 1:3) obstructive 시사!
•
첫 p/ex finding보다 Bronchodilator 쓴 후에 효과가 있는지가 중요함.
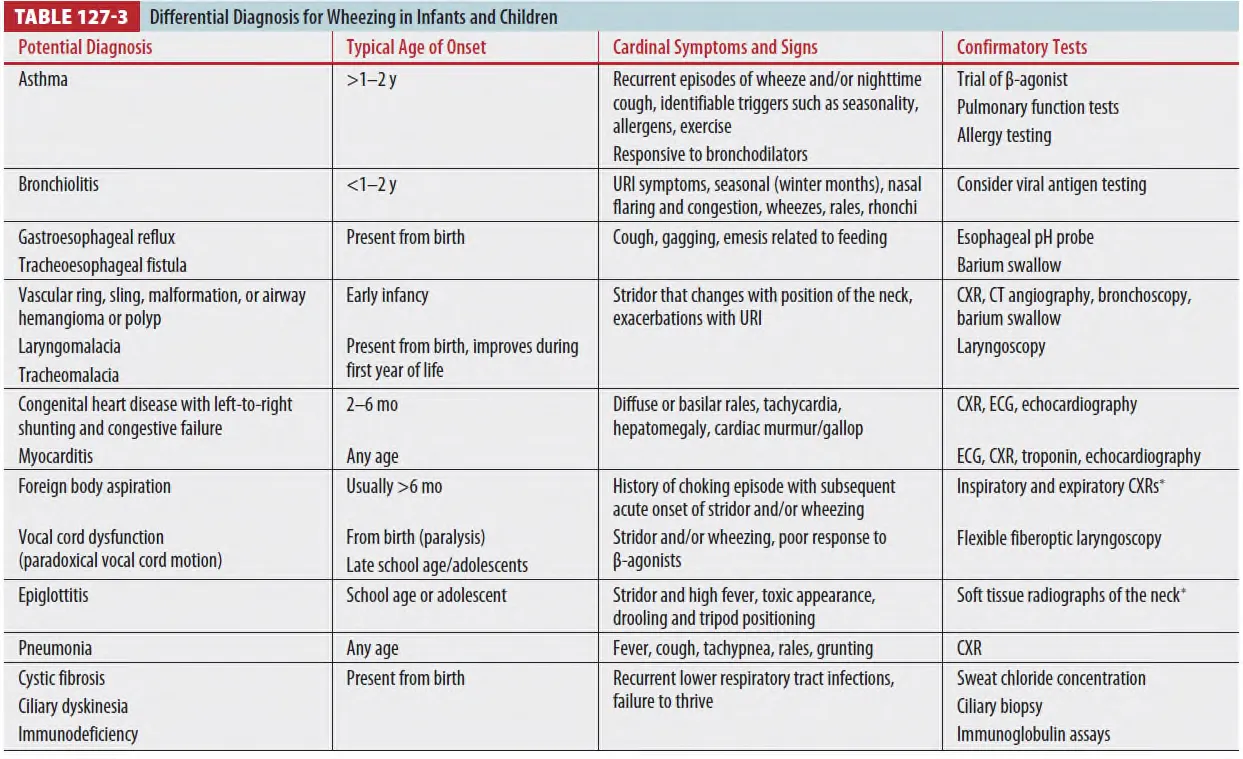
C2. Diagnosis
•
Table 127-3
(1) Asthma, bronchiolitis가 wheezing을 보이는 환아에서 진단의 대부분을 차지하나 history, p/ex,
추가 검사를 통해 다른 감별 진단들도 반드시 고려해야 한다.
(2) 이물 흡인이나 울혈성 심부전도 또한 wheezing을 유발할 수 있다.
C3. Bronchiolitis (★)
(1) 역학
•
2세 이하 환아에서 가장 흔한 하기도 감염질환
•
11월~3월에 가장 많이 발생 (북아메리카기준)
•
가장 흔한 원인 바이러스 : Respiratory syncytial virus (RSV)
그 외 : human metapneumovirus, adenovirus, influenza,rhinovirus and parainfluenza viruses
(2) 증상/징후
•
Rhinorrhea, Tachypnea, Fever, coughing
•
Use of accessory muscles, Nasal flaring, Wheezing
•
평균 7일~21일간 지속 가능. 증상은 첫 주에 가장 심함
•
아주 어린 소아에선 Irritability, cyanosis, poor feeding (WOB증가로) 증상으로 나타날 수 있다
(3) 진단
•
임상양상으로 진단한다
: 2세 미만에서 특징적 증상/징후를 보이는 경우에 의심
•
Rapid viral antigen detection도 진단에 도움이 되지 않음.
•
lab, X-ray 도 다른 질환 배제가 필요하지 않다면 routine으로 필요하지 않음.
•
Chest X-ray를 routine으로 하지는 않지만 severe hypoxia가 있거나 pneumothorax가 의심될
때는 시행을 고려해볼 수 있다.
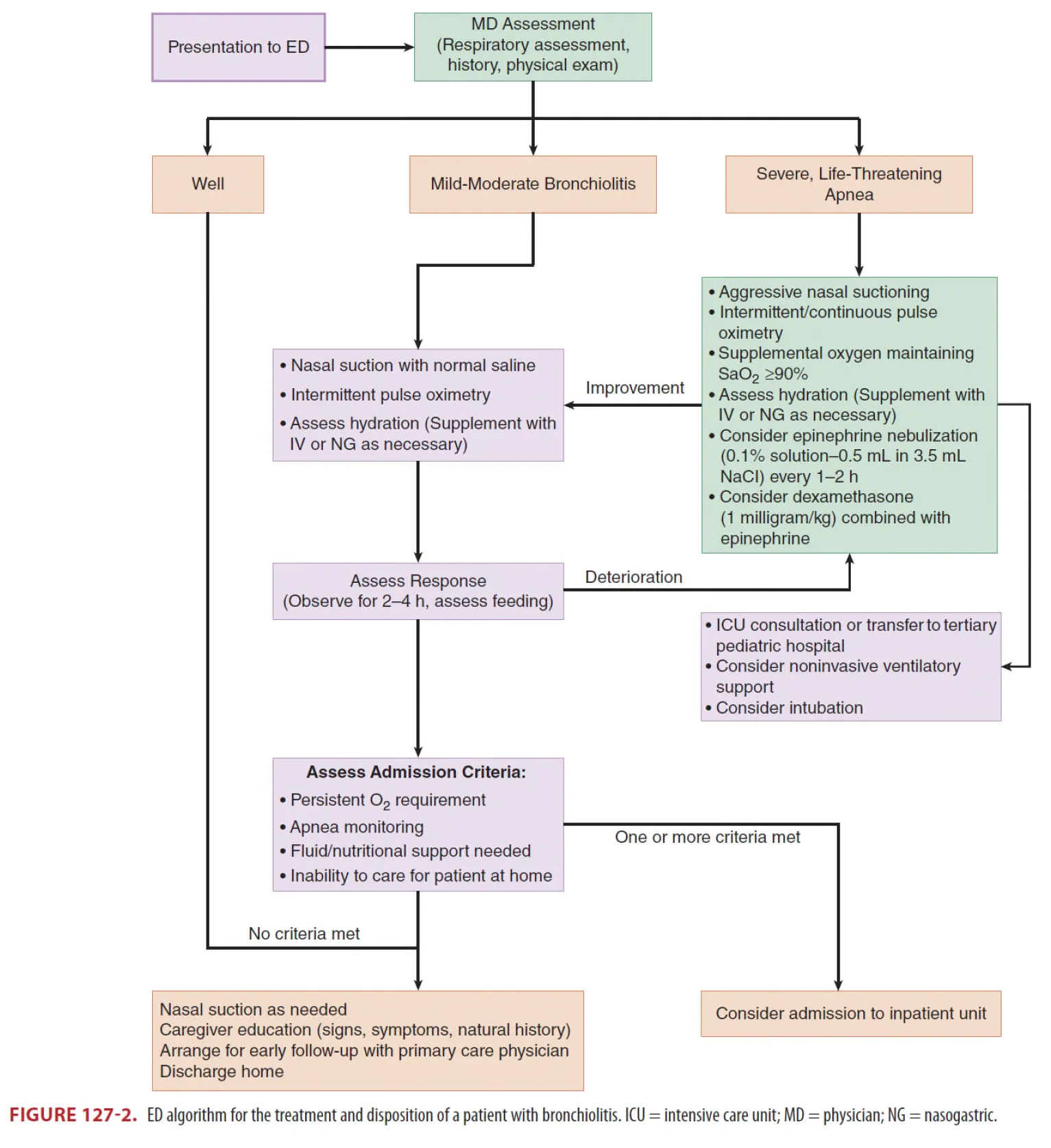
(8) 치료(★)
•
가장 중요한 Tx. : 자주 생리식염수 비강세척 및 흡인
•
β2-agonists (salbutamol/albuterol, ipratropium bromide, terbutaline) : 효과 없다.
•
Inhaled epinephrine : 입원율에는 변화 없으나 증상 완화에 써볼 수 있다. (routine 아님)
•
Dexamethasone(1mg/kg) + inhaled epinephrine은 routine 하게 쓰지는 말 것.
•
Systemic or inhaled steroid alone도 대부분 가이드라인이 쓰지 말라 되어있음
•
Nebulized hypertonic saline : 하지 마라. (d/t 2014 American Academy of Pediatrics)
•
Oxygen saturation >90% 는 유지할 것을 권고
•
NIV, HFNC는 intubation이나 MV를 줄여 주는데 도움이 될 수 있다.
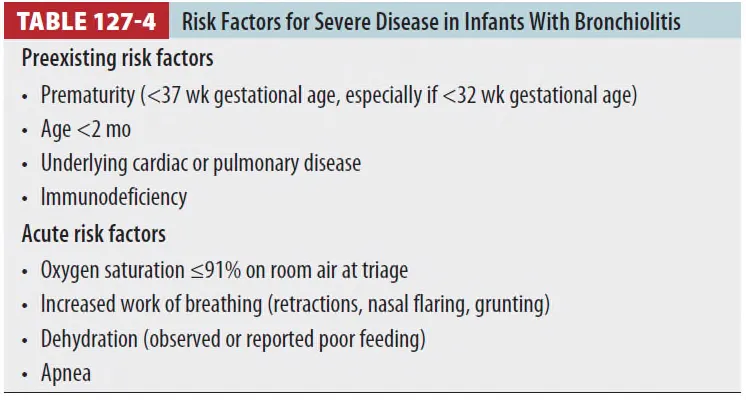
(9) 거취결정
•
대다수 환아는 퇴원 가능, 급성 악화 시 재평가 위해 재내원 당부 / 3주까지 증상 지속 가능 설명
•
Admission 적응증
: Table 127-4에 하나라도 해당하면 입원을 고려하거나 응급실에서 더 관찰하고 보내야 한다.
C4. Asthma
(1) Chronic disease,
Reversible airway obstruction d/t bronchial smooth muscle hyperreactivity and inflammation.
(2) Response to bronchodilator and Steroid Tx.
(3) Pathophysiology - 크게 3가지 process
① Inflammation ② Bronchospasm ③ Airway obstruction
(4) Clinical features and initial assessment
① 2~18세의 환아 중 95% 이상이 wheezing, shortness of breath, fever, cough, and/or dyspnea
등을 보인다.
② Pulse oximetry로 모니터하는 것을 권고, Target 93%~98%.
너무 O2 많이 주면 Hypercapnia 생김.
③ End-tidal carbon dioxide (ETCO2) monitoring 하는 것이 좋다.
정상은 35 to 40mmHg (Asthma 환자는 정상수치보다 낮아야 정상이다.)
④ 조용한 폐음은 오히려 severely compromised ventilation 시사할 수 있으며
wheezing을 만들어내지 못할 정도로 불충분한 air flow를 의미할 수 있다.
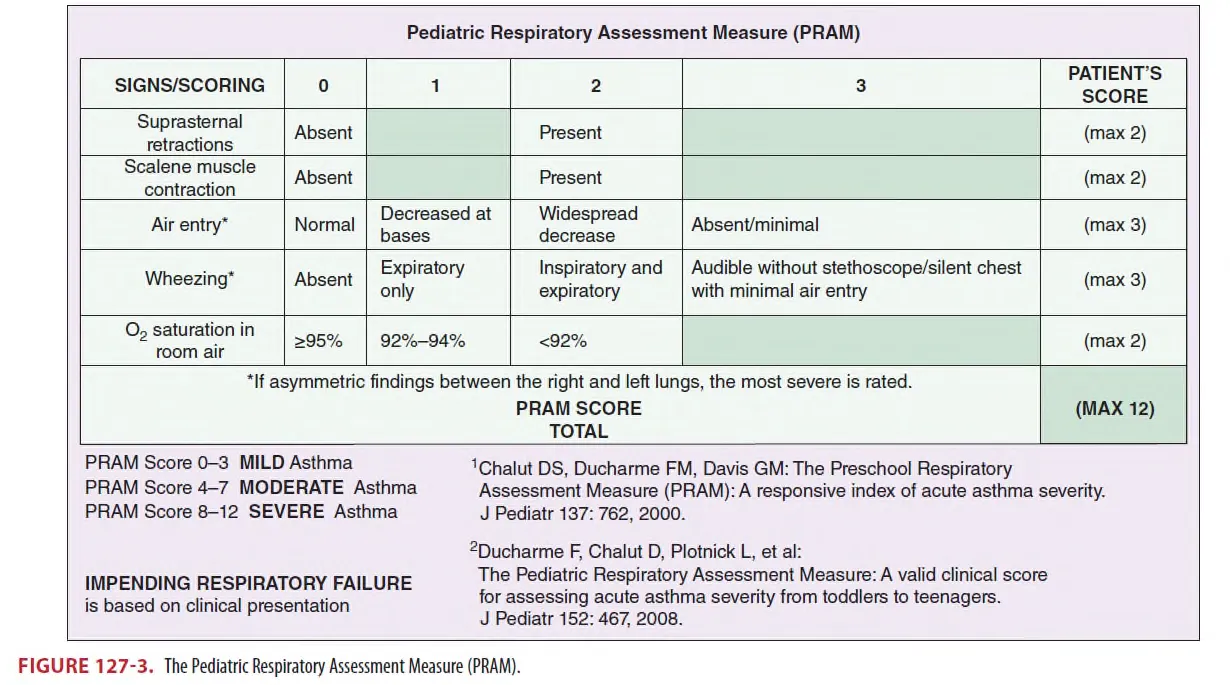
⑤ Severity : mild, moderate, severe or imminent respiratory failure (Fig 127-3)
(5) Diagnosis
① Asthma 진단 받은 바 없는 2세 이상 환아는 즉시 임상진단을 내린다
: Wheezing, Shortness of breath, Cough, Dyspnea, Diminished air entry or retractions
AND
Demonstration of reversibility with β2-agonist bronchodilators (e.g.salbutamol/albuterol)
② 1세~2세 viral-induced wheeze : asthma 또는 bronchiolitis로 치료
③ <1세 환아는 Bronchiolitis로 간주.
④ Spirometry 쓸모 있지만 <6세 환아에서 사용 힘듦, 증상이 심하면 불가,
⑤ 천식의 급성악화에 Atelectasis는 매우 흔하다,
Bacterial pneumonia 매우 드물다.
그래서 table 127-5에 나오는 indication이 아니면 x-ray를 권고하지는 않음.
⑥ Indications for chest x-ray :

(6) Treatment
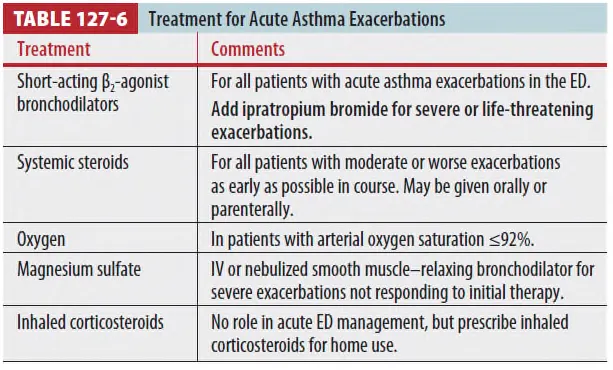
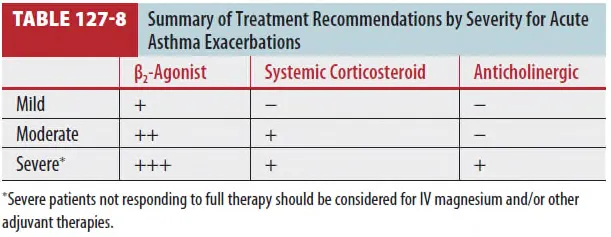
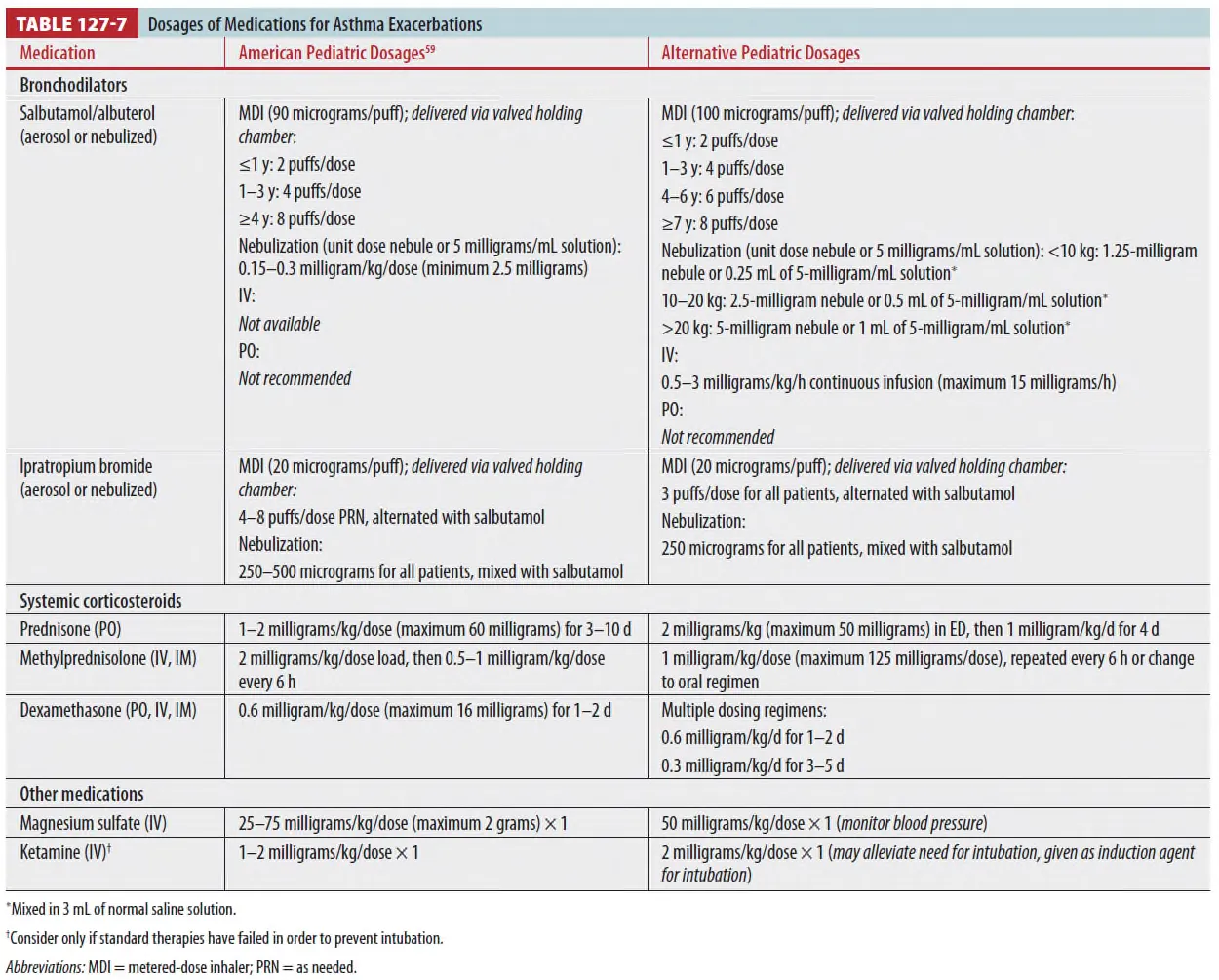



① SABA
: Salbutamol/albuterol is most widely used.
: Onset 3~5min, peak 30~120min, duration 2~5hrs
: IV dose는 air entry 너무 떨어져 도달 못할 때만
: Oral albuterol은 not recommended (delayed onset, tachycardia 등)
② Epi-pen
: β-selective medication이 없으면 써볼 수는 있는데 하기도에만 작용하는 것이 아니어서
short-term side effect를 일으킬 수는 있다.
③ Systemic corticosteroids
: Moderate, severe exacerbation 환자에게 즉시 투약되어야 한다.
: 입원률 & 재발 감소에 효과적 (Onset <4hrs)
: Triage nurse가 바로 쓰면 ED length & adm rate 감소한다.
: 내원 1시간 안에 Prednisone PO 2mg/kg 쓰고 퇴원 시 4일간 1mg/kg/d(max 60mg/d) 처방
(5 day total course) taper not required.
: Severly ill, 치료에 반응 없으면 IV methylprednisone(1mg/kg/dose) 6시간마다 추가
: Dexamethasone은 맛있음. PO, IM, IV 가능
•
Single dose (0.6mg/kg), 2day course(0.6mg/kg/d), 3~5days course(0.2-0.3mg/kg/d)
: Inhaled corticosteroid
•
ED에서 역할 없다.
•
퇴원 시 persistent 환자에게 처방 for home care
④ Anticholinergic agents(ipratropium bromide)는 SABA에 additive effect가 있다.
⑤ Mg은 bronchodilator 로 역할. IV only (nebulized 효과 없다.)
⑥ Ketamine
: Bronchodilation effect가 있어 asthma로 respiratory failure 시 induction agent로 최적이다.
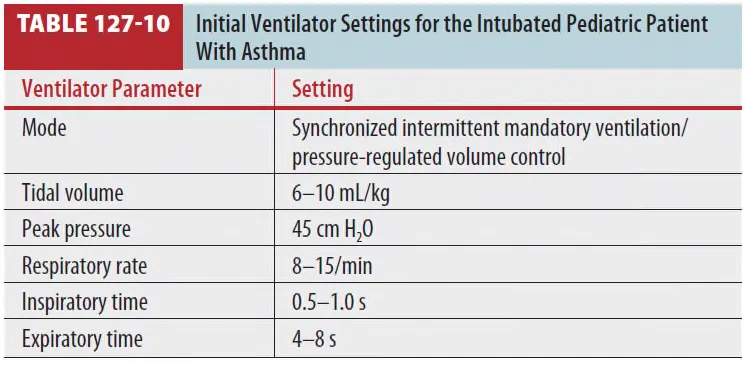
(7) Treatment of near-fatal asthma
① Noninvasive positive-pressure ventilation
: Well-fitting facemask로. 일부 tolerate하지 않은 환자에게서 sedation이 필요할 수 있음
(low dose benzodiazepine or ketamine)
: Initial setting은 severe asthma의 경우 aPEEP 12~18, PEEP 6~12로 설정
: 에어로졸 약물은 airway circuit을 통해서 주입될 수 있음
② Endotracheal intubation and assisted ventilation
: 가능한 가장 큰 직경의 appropriate cuffed ET tube를 선택
: Ketamine이 선호되는 induction agent인데 bronchodilation 효과가 있고 직접적인 BP drop을
일으키지 않기 때문
: Controlled hypercapnic hypoventilation이 추천되는 ventilator strategy이다.