Ⅰ. Definitions
•
8th에는 Sepsis, severe sepsis, septic shock의 정의가 있었으나,
9th부터는 2016 the Third International Consensus Definitions for Sepsis and Septic Shock의
정의를 소개하고 있음
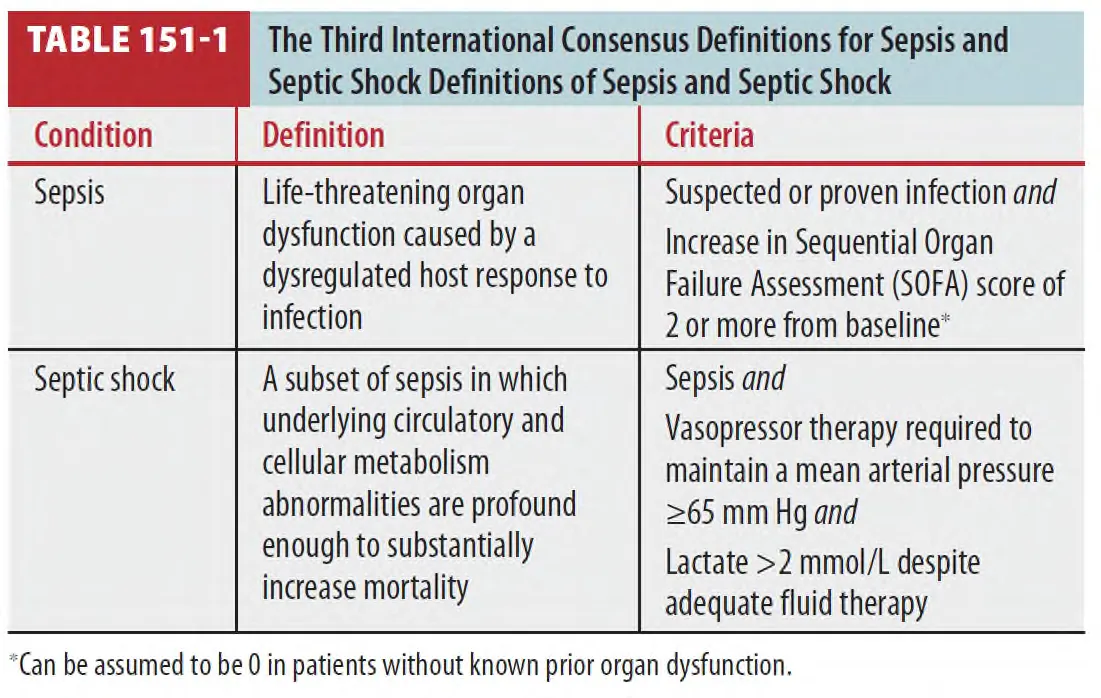
→ Severe sepsis라는 term을 제거하고 septic shock의 정의를 좁힘 (Table 151-1)
1.
Sepsis
: Suspected or proven infection, signs of systemic inflammation (엄격한 정의 없이도),
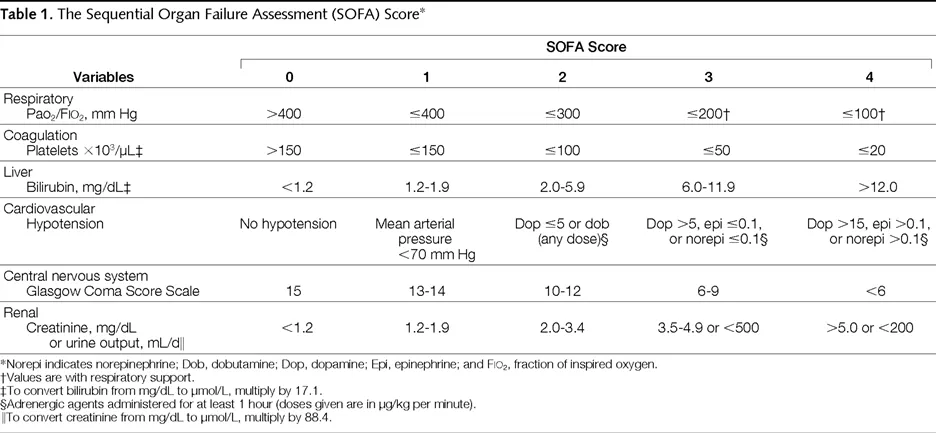
and organ failure (SOFA score 2 이상)가 있는 경우
2.
Septic shock
: Sepsis 정의에 적절한 resuscitation을 한 뒤에도 vasopressors가 필요하며 lactate level 상승한 경우
3.
International Consensus Definitions for Sepsis 새로운 정의 이전에 제정된 SEP-1의 정의는
confusing/overlapping 하므로, severe sepsis 및 septic shock 의 이전 정의를 일부 사용하였음
(1) Severe sepsis와 septic shock인 환자 : 인식부터 3시간 이내 필요한 조치
① Lactate 측정
② 항생제 투여 전 Blood and other cultures
③ 특정 원인균 target 혹은 광범위 항생제 치료
④ 30mL/kg의 crystalloid를 통한 초기 수액 치료 (60kg 일 시 1.8L)
⑤ 만약 초기 lactate 수치가 상승한 경우 (>2 mmol/L), 6시간 이내 lactate 재측정
(2) Septic shock인 환자에서 필요한 추가 조치
① Persistent hypotension 시 20mL/kg fluid bolus를 반복
② Persistent hypotension 시 vasopressor 시작
③ 임상양상과 혈역학/산소포화 측정을 통한 volume status의 적절성 및 tissue perfusion
interventions 을 판단하여 Reassessment and documentation 한다
(3) 최근 변화된 SSC(Survival Sepsis Campaign) guide line : Hour-1 bundle
① Lactate 측정
② Blood culture
③ Broad-spectrum antibiotics
④ Hypotension이나 lactate>4mmol/L일 시 30mL/kg 수액 시작
⑤ 수액을 주거나 준 이후 MAP>65mmHg 유지하기 위한 vasopressor 시작
→ 그러나 1시간 내 하는 것이 명확한 근거는 없으며 아직 널리 채택되지는 않음
(4) 8th 기준의 sepsis의 정의
① Sepsis
: Suspected or confirmed infection with evidence of systemic inflammation
(Demonstrated either through evidence of the systemic immune response syndrome or
laboratory abnormalities)
② Severe sepsis
Sepsis
•
evidence of new organ dysfunction thought to be secondary to tissue hypoperfusion
③ Septic shock
: Exists when cardiovascular failure occurs and carries the worst prognosis
•
8th에 있던 표가 9th에서는 삭제되었으나 이해를 돕기 위해 실었습니다, 참고하십시오.
Ⅱ assessment (qSOFA)
•
Score ≥2 시 high risk for poor outcome을 예측
1.
Altered mental status GCS<15
2.
Respiratory rate ≥22 breaths/min
3.
Systolic blood pressure ≤100 mmHg
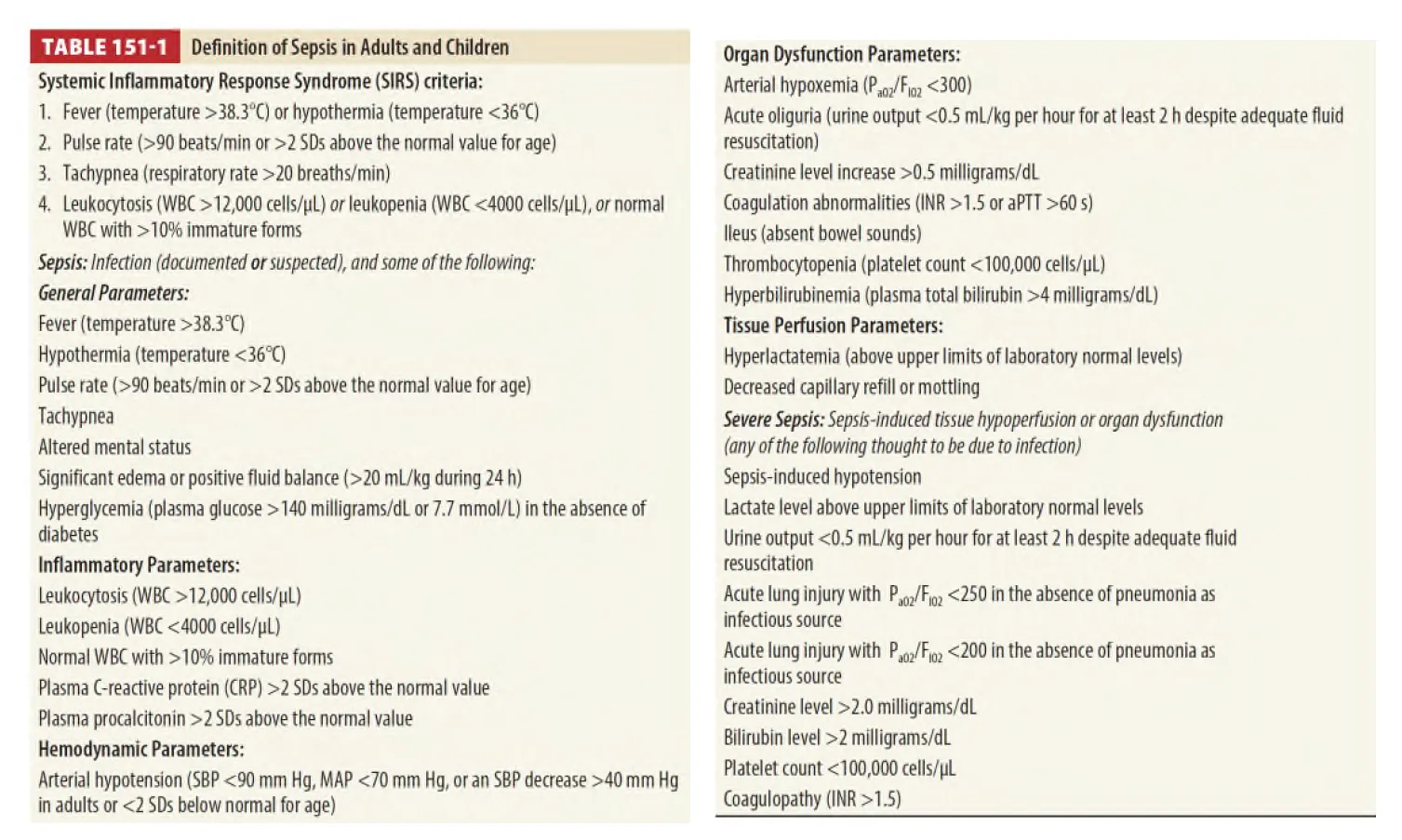
Ⅲ. Systemic inflammatory response syndrome (SIRS) Prognosis
1.
SIRS → not a diagnosis or a good indicator of outcome
(1) It is a crude means of stratification of patients with systemic inflammation
(2) Fever (BT>38℃) or hypothermia (BT<36℃)
(3) HR >90 or >2 SD above normal range
(4) RR>20
(5) WBC>12000 or <4000 or >10% immature forms
2.
Lactate : 예후인자이기는 하나 패혈증을 진단하거나 배제하는 단일 검사는 아님
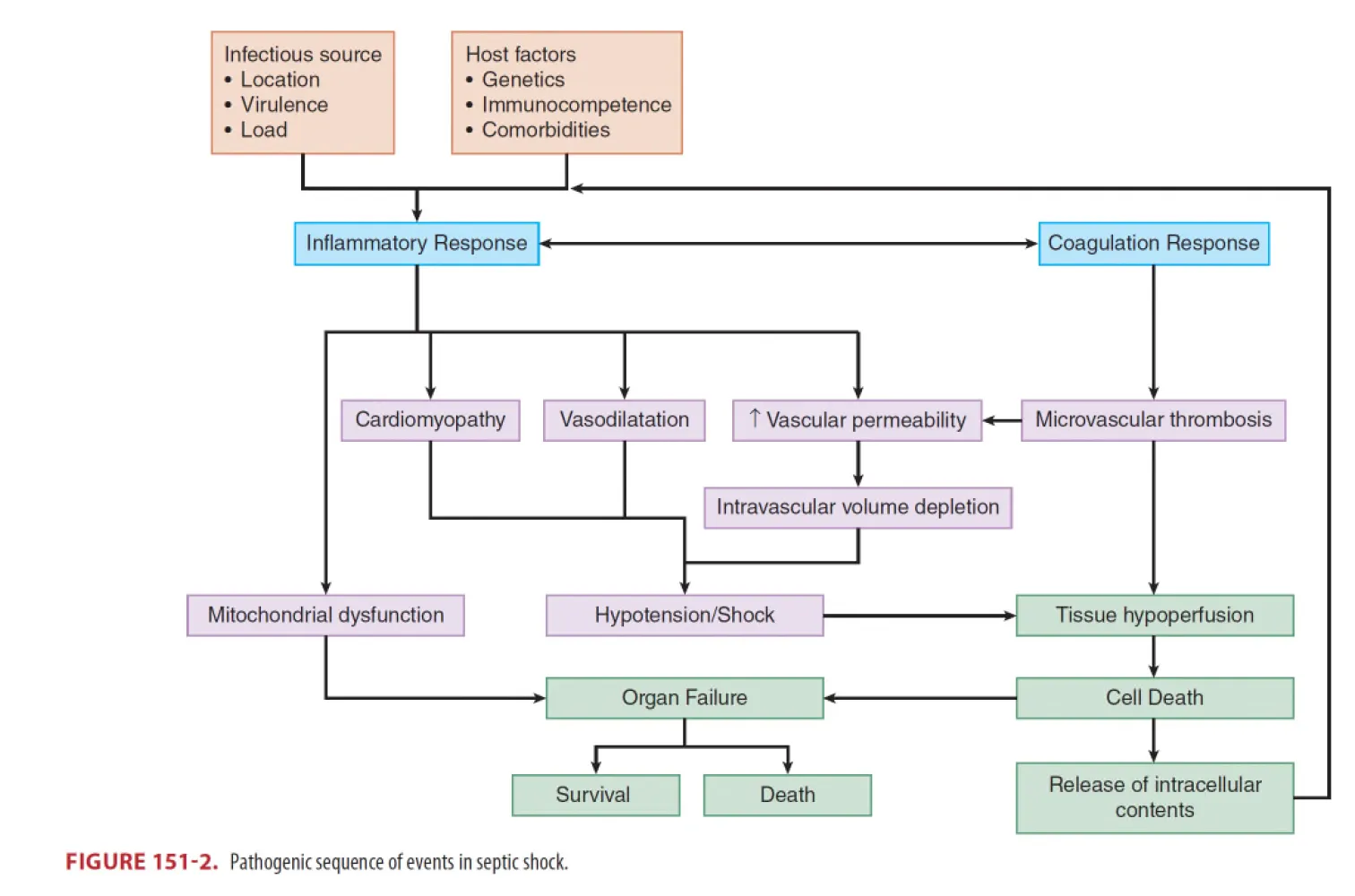
Ⅳ. Pathophysiology
•
Figure 151-2 (Pathogenic sequence of events in septic shock)
: Warm shock
•
Peripheral vasodilatation and increased cardiac output에 근거한 전통적인 shock 발생 기전
: Cold shock
•
Intravascular volume depletion and septic cardiomyopathy에 의한 shock 발생 기전
1.
Pulmonary injury : ARDS
2.
Renal injury : AKI, Azotemia, Oliguria, Anuria
3.
Hepatic injury : ALT, ALP, bilirubin 상승 (심한 상승 시는 biliary source infection 고려)
4.
GI changes : Ileus (Upper GI bleeding은 드물다)
5.
Hematologic changes : Neutropenia, neutrophilia, thrombocytopenia, DIC
6.
Metabolic changes : Lactate metabolism, hyperglycemia, adrenal insufficiency
7.
Skin : Cellulitis, erysipelas, and fasciitis, toxic shock syndrome
Ⅴ. Diagnosis
1.
Sepsis : a clinical diagnosis
2.
High frequency of sepsis in ED patients with undifferentiated shock (40%)
: 원인이 모호할 땐 septic shock을 생각하라
3.
Sepsis가 진단되었다면 source를 찾되 resuscitative measures and antimicrobial intervension을
지연시키지 않는다
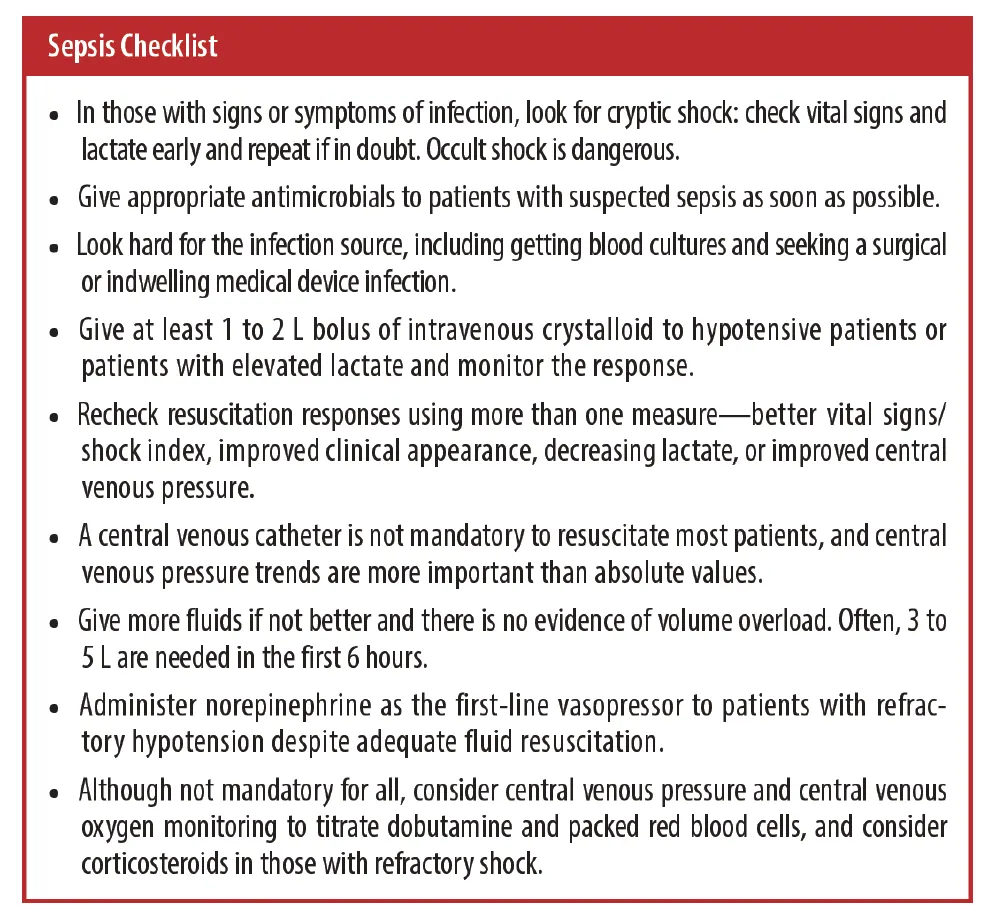
Ⅵ. Treatment
•
치료의 핵심은 early recognition, early reversal (or prevention) of hemodynamic compromise,
and early infection control이라고 강조
→ Sepsis의 빠른 인지, 적절한 초기 수액 치료, 광범위항생제 투여, 승압제를 투여, 순환의 적절성 평가가
중요하며, 혈압이 volume에 반응하지 않거나 volume overload가 예상될 경우 승압제를 바로 시작한다.
1.
Volume resuscitation
(1) Crystalloids (saline, lactated Ringer’s solution), 20~30ml/Kg bolus
가 를 덜 (2) Balanced fluids (such as lactated Ringer’s) AKI 유발하며 수액 대량 투여 시 선호됨
(3) Colloid는 초기 패혈증 치료에 불필요
(4) Hydroxyethyl starch는 AKI risk 증가
(5) Physiologic or hemodynamic response를 보이지 않는다.
판단될 때까지 crystalloid bolus를 주면서 volume expansion 필요성을 평가
2.
Vasopressor
(1) Mean arterial pressure (>65mmHg), systolic blood pressure (>90mmHg) 목표
(2) Norepinephrine : best first choice
(3) Vasopressin : Second-line agent, NE의 용량을 낮출 수 있음
(4) Epinephrine : 1~20 microgram/min으로 titration 할 수 있는 경우 norepinephrine과 동등한
안정성과 효과를 보임
(5) Dopamine은 부정맥과 심부전의 위험으로 더 이상 권고되지 않음
3.
Central venous oxygenation
Routine 하게 필요하지는 않으나 SCVO2 <70% 시 relative oxygen supply and demand mismatch를
의미함
4.
Lactate clearance
(1) Serum lactate level은 tissue perfusion을 반영하여 lactate level 감소는 적절한 tissue perfusion
회복을 시사 → 1~2시간 간격으로 lactate level check
(2) 10% 이상의 감소는 clinical outcome을 증가 시킨다
5.
Treat infection
(1) Severe sepsis 경우 broad-spectrum antibiotics 가능한 빨리 투여
(2) Outcome : Combination antibiotic therapy > monotherapy
(3) Vancomycin : 초기용량 20~30mg/kg
(4) 면역억제환자의 경우 항진균제/항바이러스제 고려
(5) SSC recommendation : Severe sepsis 확인 후 이상적으로 1시간 안에, 적어도 triage 이후 3시간
안에는 투여를 권장 (근거는 없으며 널리 채택되지 않음)
(6) 항생제 우선 투여와 우선적 hemodynamic 안정화에 대해 어떤 것이 우월한지는 분명하지 않음
(7) 이상적으로는 항생제 시작 전 모든 infectious source sample과 blood culture를 얻되 culture를
하기 위해 항생제 투약을 지연하지 말아야 함
(8) 환자가 안정화되면 잠재적인 surgical source 및 indwelling vascular line과 device도 제거
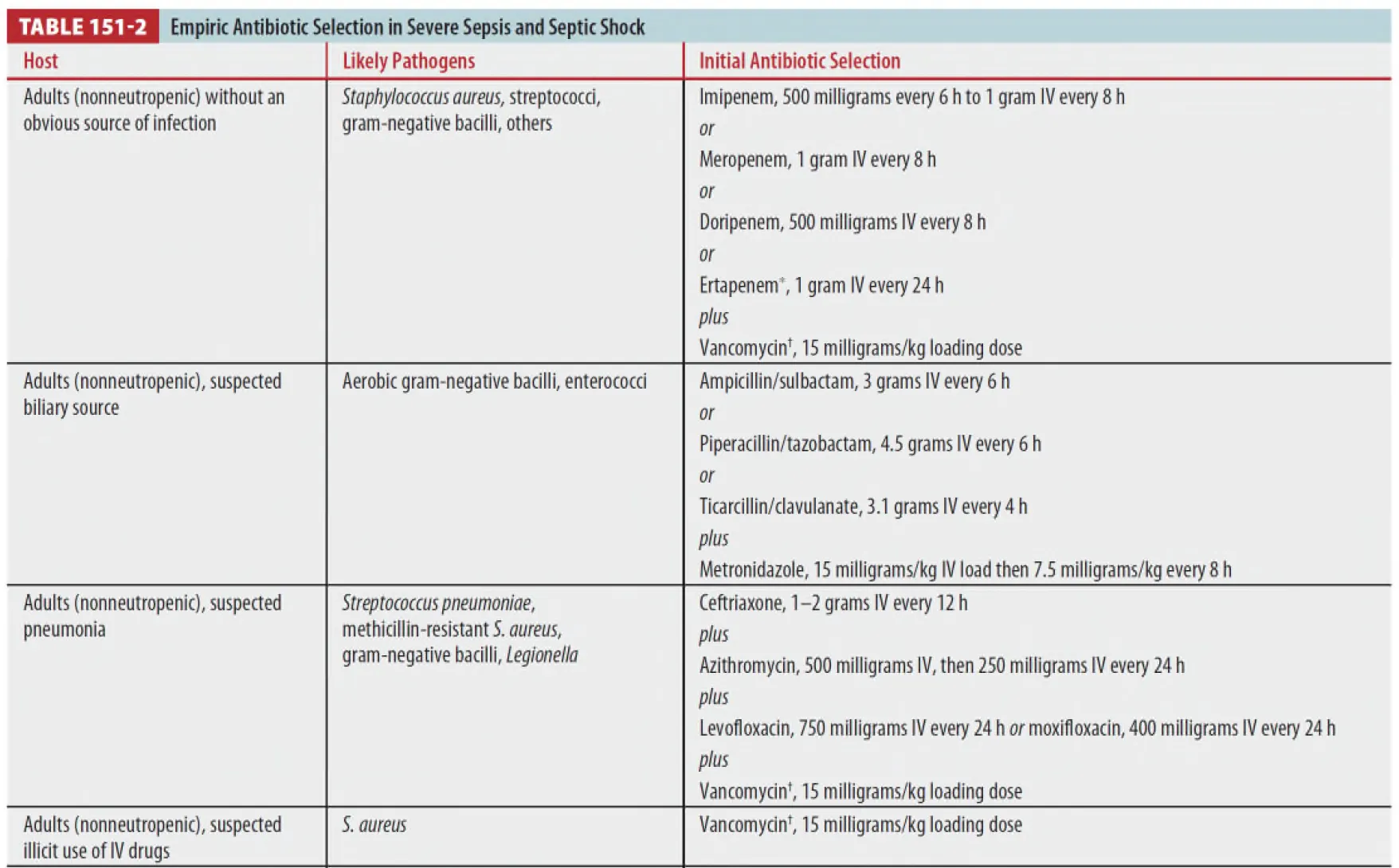
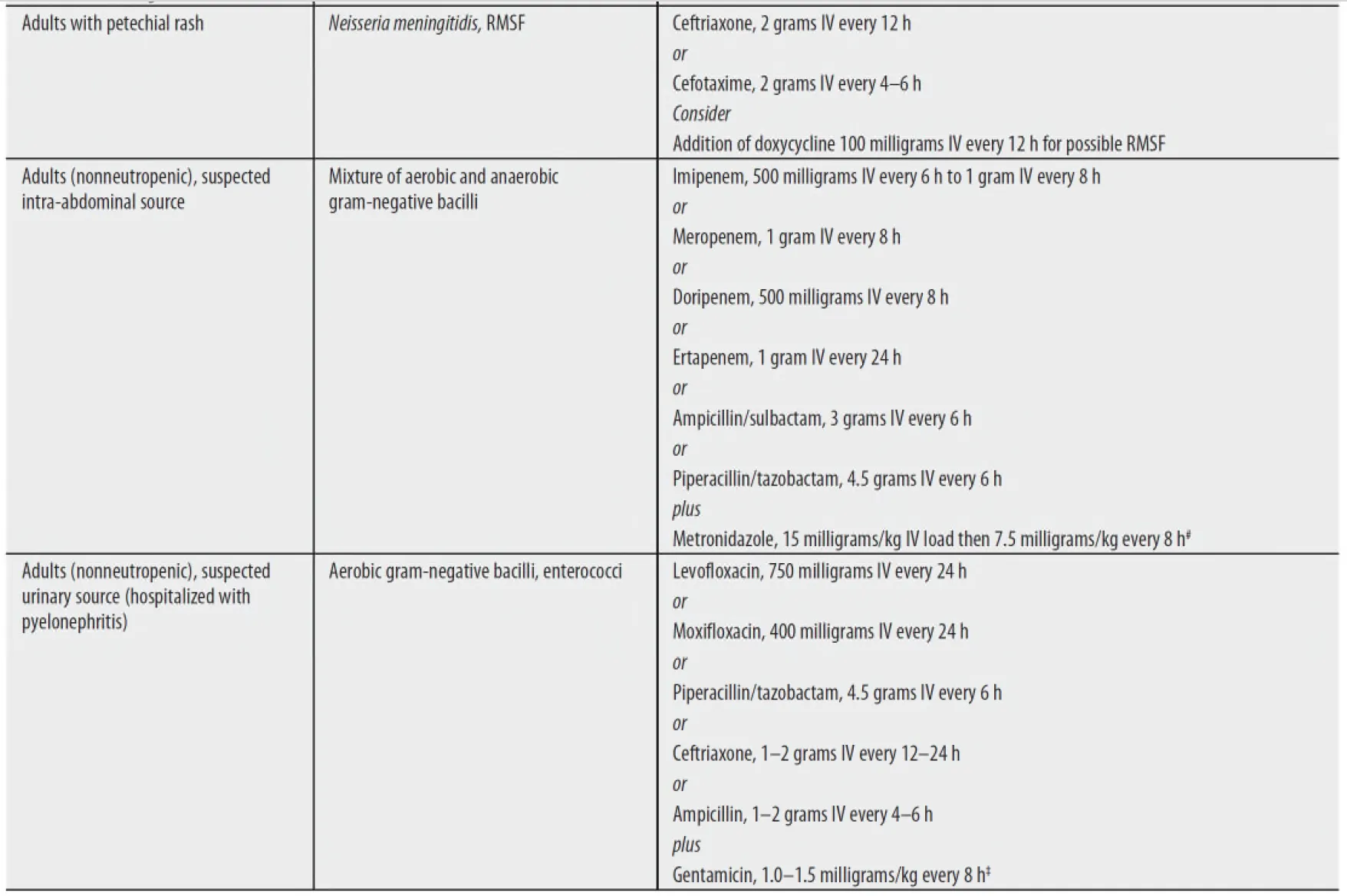
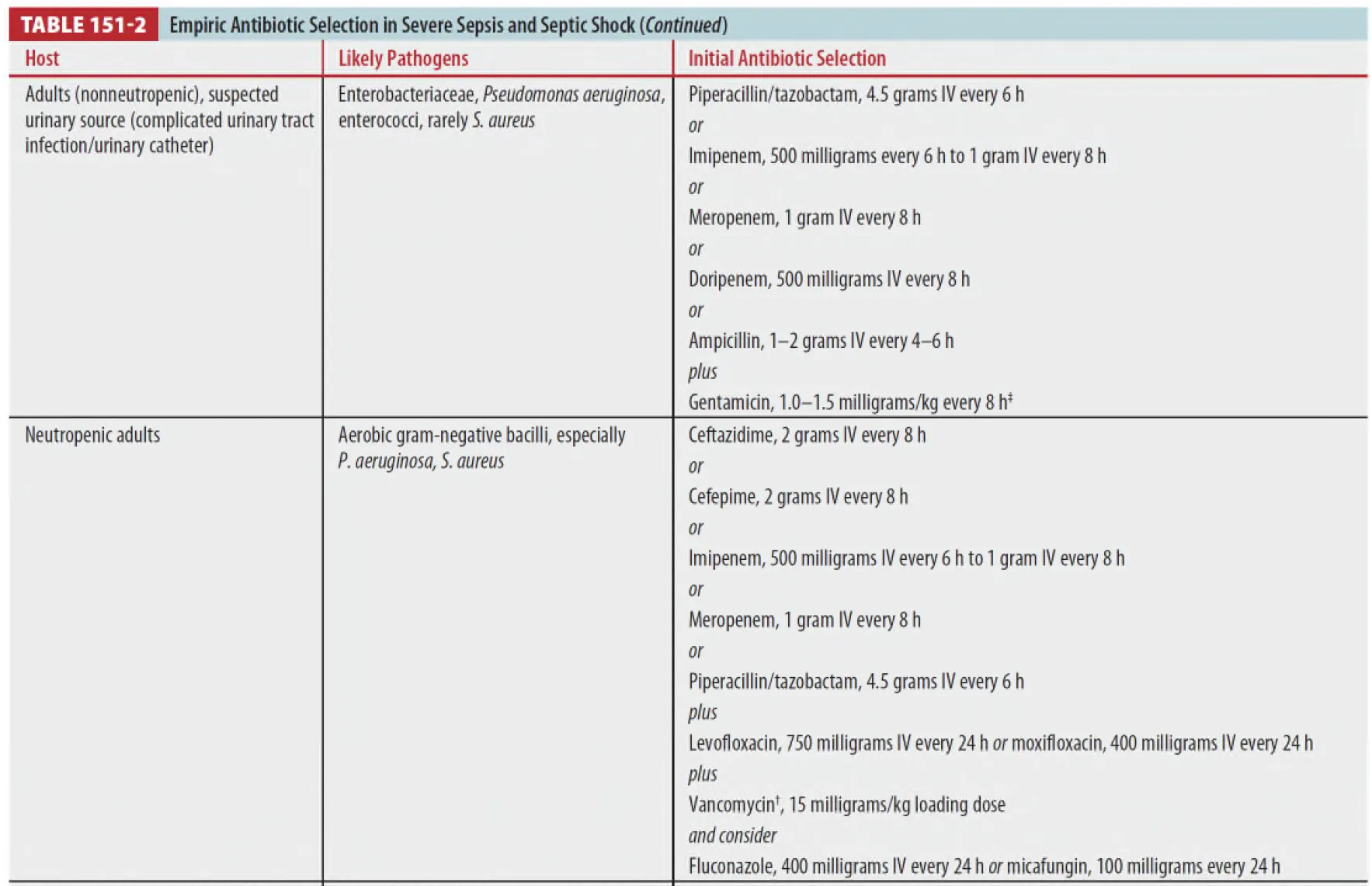
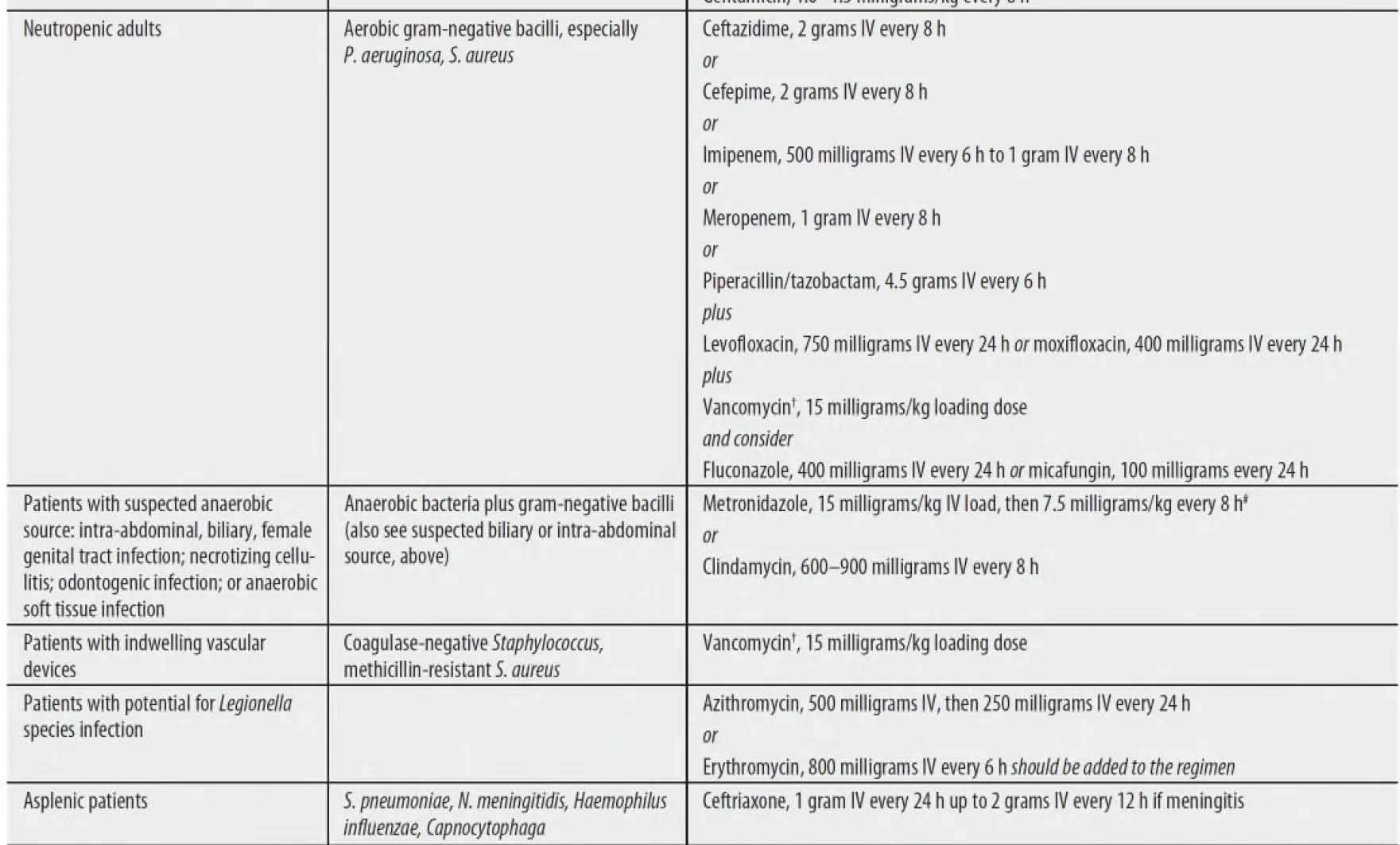
(9) Recommendation for antibiotic regimens (table 151-2)
6.
Other therapies
(1) Ventilation : Low tidal volume ventilation (6mL/kg IDW) with PEEP이 추천
(2) Glucose control : Hyperglycemia는 sepsis 예후 악화와 연관
→ Tight control (<110mg/dL)은 더 이상 권장되지 않음, modest control (<180mg/dL)
(3) Activated protein C : Sepsis의 예후에 영향을 미치지 않아 더 이상 사용되지 않음
(4) Systemic corticosteroid
① Refractory hemodynamic shock
② MV care 환자에서 shock reversal time을 줄일 수 있지만 일관된 이점이 입증되지는 않음
•
Survivng sepsis Guidelines 2017
1.
Fluid : at least 30cc/kg in first 3hr even in ESRD, CHF. use crystalloids, consider 5%
albumin avoid starch solutions.
2.
Vasopressor : Use norepinephrine (NE), avoid dopamine, add Epinephrine
if NE inadequate, add vasopressin to taper
3.
Steroid : No steroid, unless shock refractory to adequate fluids and vasopressors
4.
Antibiotics : Broad-spectrum (Vancomycin + Tapimycin), avoid double coverage.
5.
pRBC : only if Hb<7.0g/dl in the absence acute bleeding, MI, etc
6.
Source control ASAP
7.
Ventilator : TV 6cc/kg, plateau pressure≤30cmH2O, BiPAP role unknown
8.
Goal therapy : Target MAP 65mmHg, normalize lactate, glucose <180mg/dL