
A. 대후두신경 차단의 효과
대후두신경 차단은 경추성 두통(cervicogenic headache), 후두신경통(occipital neuralgia), 군발성 두통(cluster headache) 환자에게 신속하고 지속적인 통증 완화를 제공한다.
또한 NSAID 과다 사용으로 인한 두통 및 긴장형 두통에도 효과가 있다는 일부 증거가 있다.
대후두신경은 대개 **승모근(trapezius muscle)**과 **머리반가시근(semispinalis capitis muscle)**이 후두골(occipital bone)에 부착되는 부위에서 압박되거나 염증이 발생하는 것으로 알려져 있다.
ONB는 다른 치료법에 실패한 난치성 두통에 더 일반적으로 사용됨.
메타분석에 따르면 후두신경통, 편두통, 군발성 두통에 대한 임상시험과 사례 보고에서 ONB가 TTH와 함께 성공적인 것으로 나타남.
후두신경 차단술(ONB)은 후두신경통, 편두통, 경막천자 후 두통, 경추성 두통, 군발두통, 이명 및 이통과 같은 질환의 치료로 문헌에 잘 기록되어 있는 획기적인 차단술임
B. 영상을 이용하지 않는 후두신경차단술
기본 출발점은 뒤통수점(inion, external occipital protuberance)이다.
큰뒤통수신경은 뒤통수점 아래 3 cm, 측방 1 cm 부근에서 머리반가시근 사이를 뚫고 나와서, 측상방으로 이행한다. 이후 위목덜미선에 부착되는 승모근과 흉쇄유돌근의 건막 사이를 통과한다. 이 건막사이에서 큰후두신경이 통과하는 부위는, 성인의 경우 뒤통수점에서 측방 3-4 cm에 위치한다. 그러므로 큰뒤통수신경의 차단은 이 경로에서 쉽게 시행할 수 있다

1-2% 리도카인 2 mL 정도를 사용하면 신경차단은 쉽게 이루어진다.
3 ml bupivacaine 0.5% without epinephrine
3 ml of lidocaine 1% without epinephrine
국소마취제를 이용한 큰뒤통수 신경의 신경차단술 후 한, 두 시간 정도 후두두피의 감각저하가 발생해야 정확한 신경차단술이라 할 수 있다.
만약 일시적인 감각저하가 두피에 발생하지 않았다면, 국소마취제 투여가 부정확했다고 다시 시행해 보아야 한다.
뒤통수점에서 측방 2 cm, 아래 2 cm가 통상적인 랜드마크이나,
뒤통수점 3 cm 아래, 1 cm 측방 지점도 추천
1.
환자가 동의를 하고 심장 모니터에 앉으면 ONB를 적용하기 전에 목을 약간 구부린 채 앉거나 엎드린 자세로 환자를 눕힘
2.
그런 다음 환자가 통증을 가장 많이 호소하는 머리 측면의 후두 돌기와 유양돌기를 촉진함
3.
대후두신경은 후두 돌기에서 약 2cm 아래, 후두 돌기에서 약 2cm 옆으로, 후두 돌기에서 유양돌기까지의 거리의 약 3분의 1에 위치함
4.
니다. 의사는 골막과의 접촉을 나타내는 저항이 느껴질 때까지 후두부를 향해 90도 각도로 25G를 전진
5.
그런 다음 바늘을 약 1mm 빼고 후두동맥에 바늘이 없는지 확인하기 위해 흡인
6.
이 차단술의 경우, 음성 흡인 후 마취제 3mL를 신경 주위에 부채꼴 모양으로 서서히 주입한다
7.
두피의 풍부한 혈관 공급으로 인해 바늘을 빼낼 때 마취제에 신경을 담그고 지혈을 위해 압력을 가해야 함
8.
양쪽 후두 신경을 적절히 마취하고 가장 적절한 통증 완화를 제공하기 위해 양측으로 시행
9.
환자가 보고한 평균 통증 완화 시간은 15분임
10.
두피의 이질통을 보고하고 GON 촉진으로 재현할 수 있는 통증이 있는 환자는 ONB를 받은 후 원하는 수준의 진통 효과를 얻을 가능성이 가장 높다
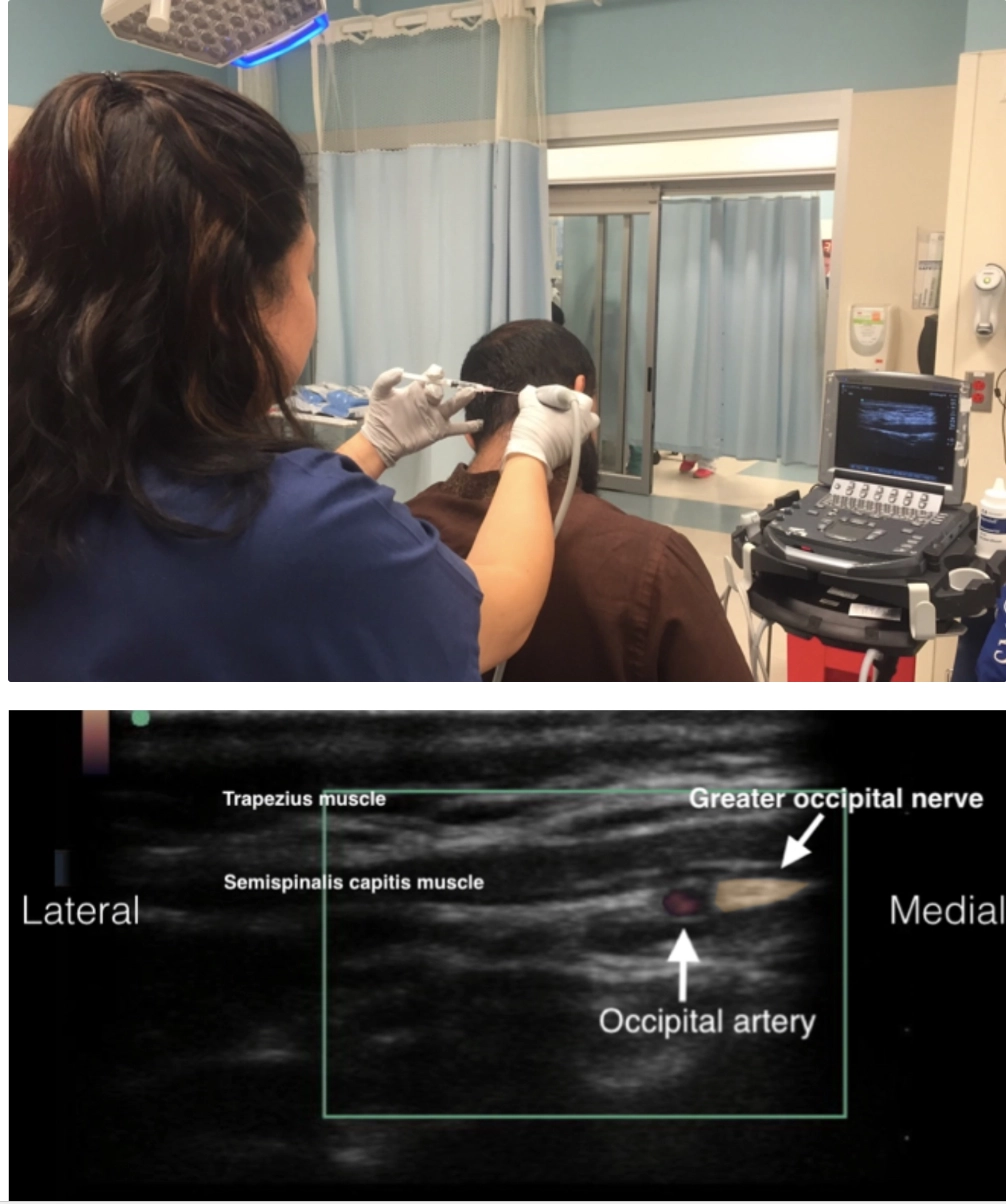
C. 초음파 유도 하 시술 방법
C1. 환자 자세
•
환자는 머리를 약간 앞으로 숙인 상태에서 앉거나, 엎드린 자세로 위치할 수 있습니다.
C2. 해부학적 구조 찾기
•
상항선(superior nuchal line)을 따라 촉진하여 후두동맥(occipital artery) 맥박을 느낄 수 있는 부위를 찾습니다. 이는 일반적으로 inion(후두골 융기)에서 약 3cm 가쪽에 위치함.
•
대후두신경은 후두동맥의 안쪽(medial)에 위치.
C3. 초음파 유도 절차
초음파 탐촉자 배치:
•
직선형 탐촉자(linear probe)**를 횡단 방향으로 inion의 가쪽 상항선 위에 배치함.
•
초음파 화면에서 맥동하는 후두동맥을 식별하고, 컬러 도플러(Color Doppler)를 이용해 확인함.
•
후두동맥의 안쪽에서 대후두신경을 흰색 다발처럼 관찰할 수 있다.
C4. 주사
•
1% 리도카인 또는 1% 리도카인과 0.25% 부피바카인(bupivacaine) 혼합액(50:50)을 1~3mL 주입한다
•
주입 시 신경 섬유 다발(fascicle)에 직접 주입하지 않도록 주의한다.
•
환자는 통증이 빠르게 개선되는 것을 경험하게 된다.
•
일부 연구에서는 시술 후 최대 4주 동안 통증 완화 효과가 지속될 수 있다고 보고했다.
