

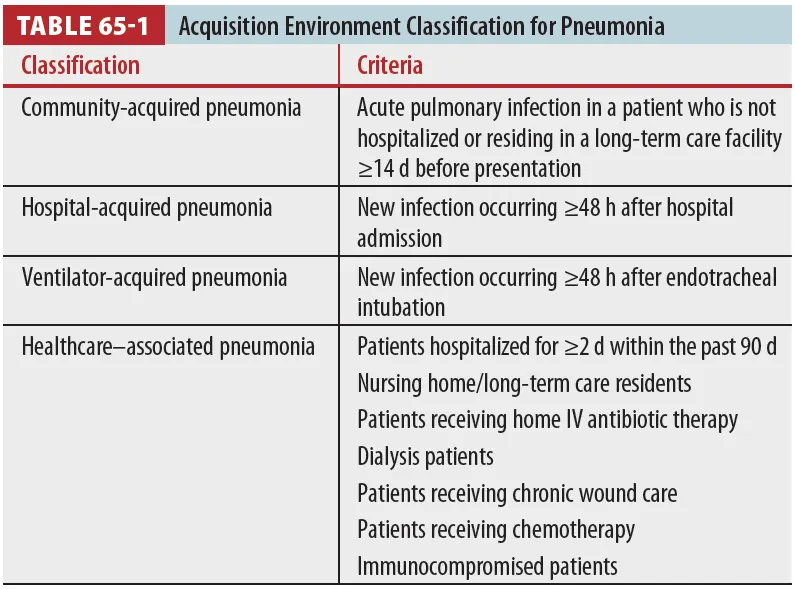
A. Pneumonia classification criteria
B. Pathophysiology
1.
Pneumonia risk factors (Table 65-2)
(1) Aspiration risk : 삼킴/식도운동장애, 뇌경색, NG tube, Intubation, Seizure, Syncope
(2) Bacteremia risk : Vascullar device 거치, Intrathoracic devices (ex, chest tube)
(3) Chronic disease : 당뇨, 신부전, 간부전, Valvular heart dz. Congestive HF.
(4) Debilitation : 알콜 중독, 고령, Neoplasia, 면역저하자
(5) Pulmonary disorders : COPD, Chest wall disorder, Skeletal muscle disorder,
Bronchial obstruction, Bronchoscopy, Viral lung infection
2.
Community acquired pneumonia
(1) Identified specific pathogen은 딱히 없는 것으로 알려져 있다.
(2) Identified pathogen 중 M/C은 Pneumococcus이고, virus, atypical agent (Mycoplasma, Chlamydophila, Legionella)가 그 뒤를 잇는다.
(3) Most severe CAP 균주는 S. pneumoniae와 Legionella로 CAP의 치료에는 이 둘을 cover 해야한다.
C. Diagnosis
1.
진단은 Sx (fever, cough, rales or rhonchi) 및 Chest X-ray confirm을 통해 한다.
2.
대부분의 환자에게서 specific organism의 동정은 굳이 필요없다.
3.
Blood 및 Sputum culture의 경우 아래 selected patient에게서 recommend
: ICU, Leukopenia, Cavity lesions, Severe liver dz., Alcoholism, Asplenia, Pleural effusions.
D. Clinical features
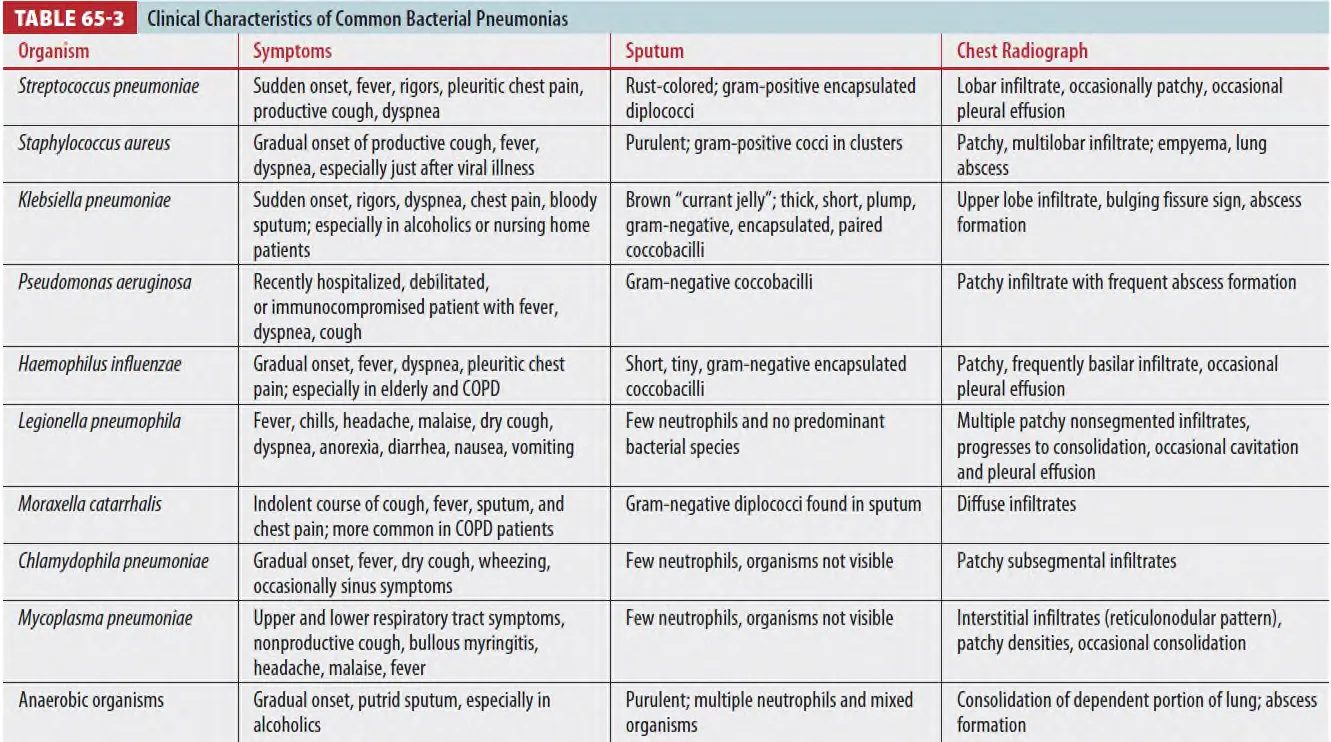
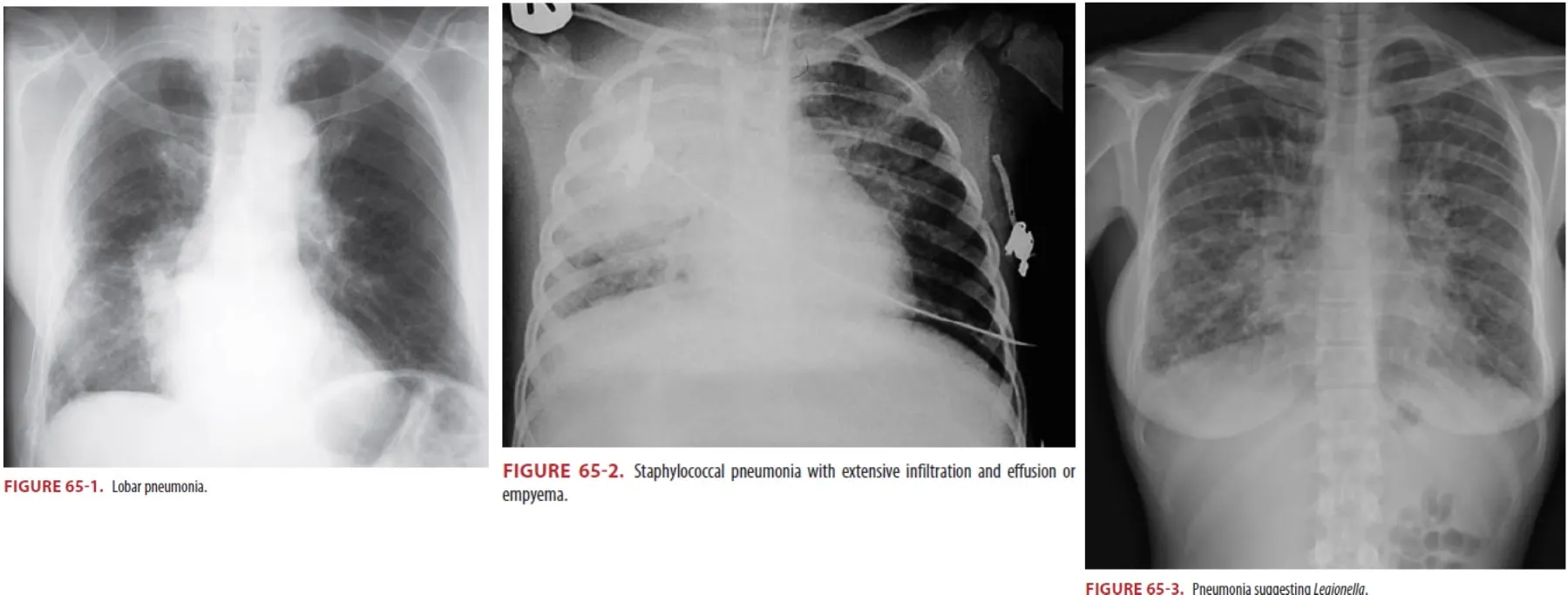
D1. Pneumococcal pneumonia
(1) Sudden onset of disease
: Rigors, Bloody sputum, High fever, and Chest pain with lobar infiltrates
(2) Responds to a variety of antibiotics, although there is penicillin-, macrolide-,and fluoroquinolone-resistant pneumococci
(3) Highly penicillin-resistant pneumococci require treatment with vancomycin, imipenem, a newer respiratory fluoroquinolone or ketolide
D2. Other bacterial pneumonias
(1) S. aureus
① Insidious onset
② Extensive and multiple infiltrates with empyema, pleural effusions
③ Healthcare-acquired pneumonia are at risk for infection with MRSA
(2) Klebsiella
① Acute onset
② Lobar infiltrate
③ In compromised patients : at risk of aspiration, alcoholics, the elderly
(3) Pseudomonas
① Bilateral lower lobe infiltrates with a prolonged hospitalization
who received broad-spectrum antibiotics or high-dose steroid therapy
with structural lung dz. (including cystic fibrosis), or who are nursing home residents.
(4) Haemophilus influenzae
Pleural effusions ① and multilobar infiltrates
with chronic lung disease, sickle cell disease, or immunocompromised disorders
and in alcoholics and diabetics
(5) Moraxella catarrhalis
① Diffuse infiltrates
② Cough and sputum production with fever and pleuritic chest pain
D3. Pneumonia from Atypical Bacteria and Viruses
•
Lack a cell wall
→ Not respond to β-lactam antibiotics
respond to macrolides or a respiratory fluoroquinolone
(1) Legionella
① No seasonality
② from benign self-limited disease to multisystem organ failure commonly complicated by
GI symptoms (abdominal pain, vomiting, and diarrhea)
(2) Chlamydophila
① Patchy subsegmental infiltrate
② Linked to adult-onset asthma
(3) Mycoplasma pneumonia
① Epidemics every 4 to 8 years
② Patchy infiltrates
③ Retrosternal chest pain. no GI symptoms
④ Extrapulmonary symptoms
(Rash, Neurologic symptoms, Arthralgia, Hematologic abnormalities, or Rarely acute kidney injury)
마이코플라스마 뉴모니아는 어린이 상기도 및 하기도 감염의 빈번한 원인이며 학령기 어린이와 청소년 폐렴의 주요 원인입니다[1]. 감염은 일반적으로 경미하고 자가 제한적이지만 경우에 따라 스티븐스존슨증후군과 독성 표피 괴사증을 모방할 수 있는 중증 점막염이 발생할 수 있습니다. 한때 마이코플라즈마 유발 발진 및 점막염(MIRM)으로 분류되었던 이 질환은 다른 감염원이 이 질환을 유발할 수 있기 때문에 현재 반응성 감염성 점막 피부 발진(RIME)으로 알려져 있습니다. RIME은 주로 약물로 인한 유발 요인보다는 호흡기 감염 후 어린이와 청소년에서 발생하며, 마이코플라스마 뉴모니아에 감염이 이 중증 점막 피부 증후군의 주요 원인으로 지목되고 있습니다[2]. 입술의 출혈성 딱지와 혀의 미란이 가장 흔합니다[3,4]. 안구 침범이 있는 환자는 종종 화농성 양측 눈 분비물, 광 공포증, 눈꺼풀 부종이 있습니다[3,4]. 비뇨생식기 병변이 발견될 수 있습니다. 피부 병변은 일반적으로 드물고 흔하지 않지만 몸통, 사지, 때때로 얼굴에서 발견될 수 있습니다. 지지적 치료 외에도 마크로라이드 항생제, 전신 코르티코스테로이드, 면역 조절 치료가 필요할 수 있지만 스티븐스-존슨 증후군 및 독성 표피 괴사에 비해 예후가 양호하고 전반적인 사망률이 낮습니다[4].

(4) Viruses : m/c influenza, seasonal
E. Pneumonia in special populations
E1. Alcoholics
(1) S. pneumoniae가 M/C pathogen Klebsiella, Haemophilus 균주가 Alcoholics 감염에 중요 균주
(2) Non-alcoholics에 비해 pneumonia 빈도가 높다.
E2. Diabetes
(1) 25~64세의 DM환자들에게서 pneumonia와 influenza의 빈도는 정상군에 비해 4배이며, 이로 인한 사망 역시 2~3배 높다.
(2) DM 환자들에게서 S.aureus, G(-)bacteria, Mucor, and Mycobacterium tuberculosis가 높은 빈도로 나타납니다.
E3. Pregnant
(1) CAP로 인한 Maternal mortality는 약 3%입니다.
(2) Varicella pneumonia가 특히 산모에게서 문제가 된다.
(3) 산모 환자라도, Respiratory tract infection의 sx이나 varicella exposure가 있으면 CXR 진행이 권고.
(4) IV acyclovir가 ED에서 시작하도록 책에서는 권장하고 있다.
E4. Elder
(1) 고령환자에서 폐렴은 M/C infection이며, Mortality rate은 40%
(2) 고령 환자에게서는 젊은 환자에 비해 Pneumococcal 감염이 3배, 이로 인한 사망률 역시 5배 많다.
(3) Influenza는 고령에서 M/C serious viral infection이며 H1N1이나 seasonal influenza 후 발생하는 postinfluenza bacterial pneumonia에서 M/C pathogen은 S. pneumoniae, S. aureus or H. influenzae입니다.
E5. Nursing Home
(1) Nursing home 폐렴 환자에서의 8가지 예측 인자는 다음과 같다.
① 분당 맥박수 상승 ② 분당 호흡수 상승 (30회/분)
③ 38℃ 이상 fever ④ Somnolence(졸림/무기력) 또는 의식 저하
⑤ Acute confusion ⑥ 청진상 lung crackles
⑦ Wheezes의 부재 ⑧ Leukocyte 상승.
(2) M/C pathogens는 S. pneumoniae, G(-) bacilli, H. influenzae이다.
(3) 이들 환자군은 Health care-associated pneumonia의 risk가 높아 치료 시 MRSA에 대한 치료가 권장된다.
E6. HIV
(1) M/C pathogens는 S. pneumoniae이며, P. aeruginosa 역시 호발한다.
(2) HIV 환자에서 세균성 폐렴 발병 시 pleural effusion이 60%에서 관찰되며 원인은 S. pneumonia와 S. aureus입니다.
E7. Transplant
(1) 세균성 폐렴이 다른 수술환자에 비해서 호발
(2) 신장이식환자다 간, 심장, 폐 이식 환자의 수술 후 첫 3개월 이내에 호발하는 경향이 있다.
(3) G(-) bacilli(주로 P. aeruginosa), S. aureus, Legionella 등 수술 후 3개월 이내에 나타납니다.
F. Treatment
(1) Typical Pneumonia의 경우
•
Pneumococcus 에 듣는 항생제 사용 (cepha, 내성균은 FQ)
•
Pseudomonas, MSSA, Tbc 가능성 있으면 coverage 범위가 넓은 항생제 고려
(2) Atypical Pneumonia의 경우
•
Viral - no Abx
•
Mycoplasma - Doxycycline (Macrolide 내성이 높아서)
•
Mostly, do not require organism identification through blood or sputum for antibiotic treatment : Respond to empiric antibiotic treatment
대부분 항생제를 위해 혈액이나 가래를 통한 유기체 식별이 필요하지 않습니다.
치료할 필요가 없습니다: 경험적 항생제 치료에 반응합니다.
백혈구 감소증, 구강 내 병변, 중증 간 질환, 중증의 간 질환, 알코올 남용, 무력증, 흉막 삼출이 있는 경우 혈액 배양 검사 실시
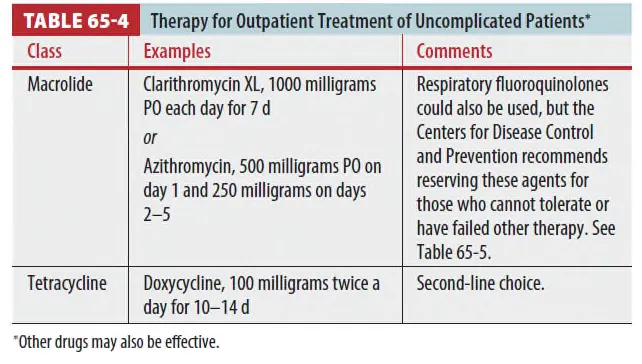
F1. OPD f/u of uncomplication
•
중증도가 낮아 외래에서 치료 가능한 환자군. 다음 항생제 중 하나를 단독으로 사용.
•
국내에서는 Tetracyclin이나 macrolide의 단독요법은 S.pneumoniae의 높은 내성으로 인해 권장 안됨. (Tinti 교과서와 다름)
<국내 Guideline>
(1) 옵션1 : B-lactam 단독 또는 B-lactam과 Macrolide 병용
•
B-lactam : amoxicillin, amoxicillin-clavulanate, cefditoren, cefpodoxime
•
Macrolide : azithromycin, clarithromycin, roxithromycin
•
비정형폐렴이 의심되는 경우 b-lactam에 macrolide를 병합

(2) 옵션2 : Respiratory FQ 단독요법
•
FQ은 결핵균에도 효과. 따라서 pul.tbc인 경우 진단이 지연될 수 있고, 내성유발 가능
⇒ 결핵 가능성이 있는 경우에는 FQ 단독요법은 쓰지 말 것.
•
Respiratory FQ : gemifloxacin, levofloxacin, moxifloxacin (not suspected Tbc)
<Tinti>
(1) Macrolide (1st) 또는 Tetracycline(2nd)을 씁니다. → 국내적용불가
•
Macrolide : Clarithromycin XL, 1000mg PO를 7d간 복용
•
또는 Azithromycin, 500mg PO on day 이후 250mg씩 2-5d간 복용
•
Tetracycline : Doxycycline, 100mg씩 하루 두 번, 10~14d간 복용.
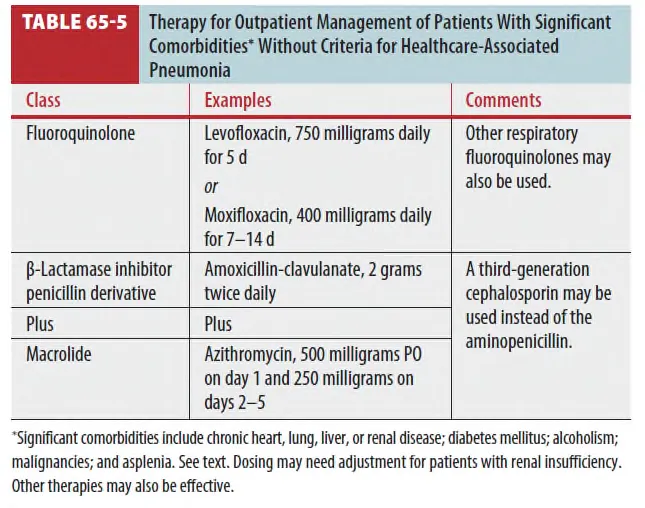
F2. OPD f/u with comorbidities
(1) 적용조건
•
Chronic Heart, lung, liver or renal dz가 있거나, DM, alcoholism, cancer, asplenia가 있는 환자
•
HAP 가 아닐 것.
•
Fluoroquinolone : Levofloxacin, 750mg, 5일간
또는 Moxifloxacin, 400mg을 7~14일간 복용
•
β-Lactamase inhibitor penicilin + Macrolide
: Amoxicilin-clavulanate 2g씩 하루 두 번
: Azithromycin 500mg PO on day 이후 250mg씩 2~5d간 복용.
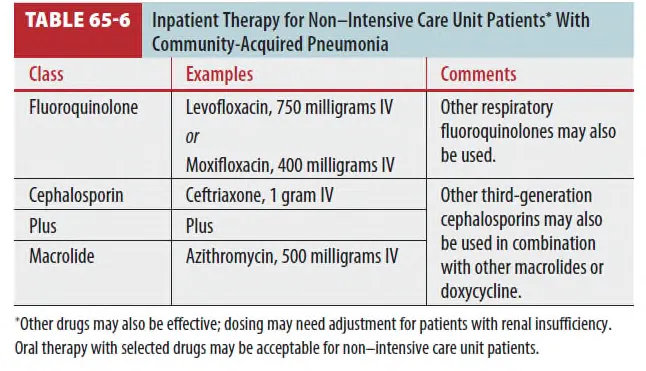
F3. 일반병실 입원환자 with CAP
<국내 Guideline>
(1) 옵션1 : b-lactam 단독요법
•
Amoxicillin/Clavulanate 1.2g IV q 6-8hr
•
Ampicillin/Sulbactam 3g IV q 6hr
•
Cefotaxime 2g IV q 8hr
•
Ceftriaxone 2g IV q 24hr
(2) 옵션2 : FQ 단독요
•
Gemifloxacin 200mg IV q 24hr
•
Levofloxacin 750mg IV q 24hr
•
Moxifloxacin 400mg IV q 24 hr
(3) 비정형 폐렴이 의심되는 경우 또는 심한 폐렴
비정형 폐렴(Mycoplasma, Chlamydophila 등)이 의심되는 경우, β-lactam에 마크로라이드를 병용할 수 있다. 다만 국내 지침상 모든 입원 환자에게 병합 요법이 단독 요법보다 우월하다는 근거는 부족하므로, 일괄 병용이 필수는 아님.
main | plus |
Amoxicillin/Clavulanate 1.2g IV q 6-8hr
Ampicillin/Sulbactam 3g IV q 6hr
Cefotaxime 2g IV 1 8hr
Ceftriaxone 2g IV q 24hr | Azithromycin 500mg PO/IV q 24hr
Clarithromycin 500mg PO/IV q 12hr |
or | |
Gemifloxacin 200mg IV q 24hr
Levofloxacin 750mg IV q 24hr
Moxifloxacin 400mg IV q 24 hr | none |
<Tinti>
(1) Fluoroquinolone 단독 또는 3rd 세파 + Macrolide(또는 doxycycline)를 사용
•
Fluoroquinolone : Levofloxacin, 750mg IV 또는 Moxifloxacin, 400mg IV 사용
•
3rd 세파 + Macrolide : Ceftriaxone, 1g IV + Azithromycin, 500mg IV
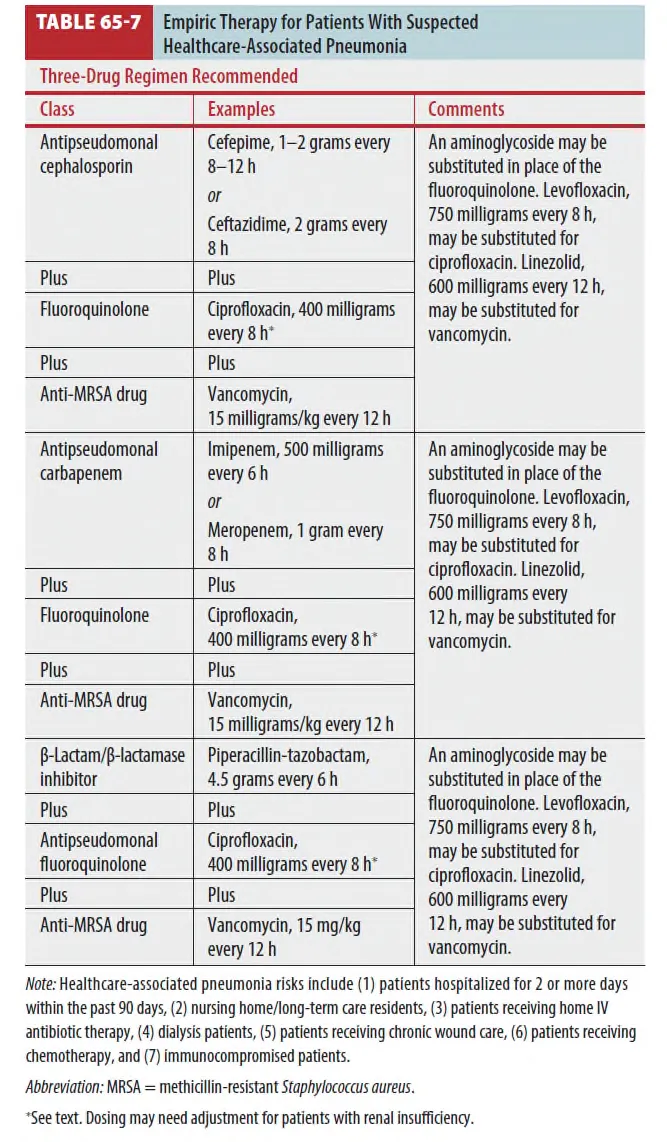
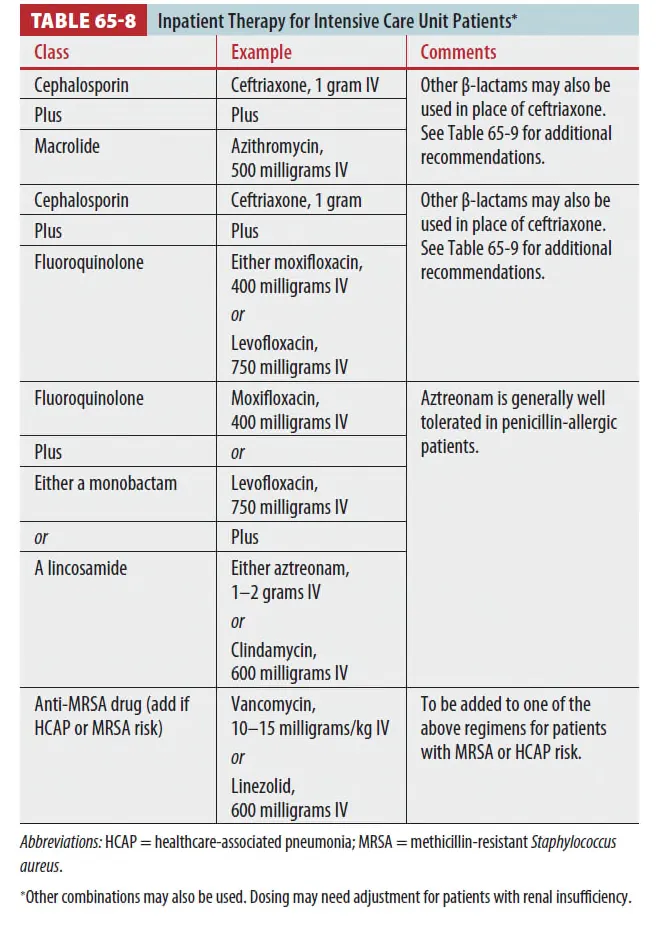
F4. 입원환자 with Health Care-associated Pneumonia
(1) 이들 환자군에서는 다음과 같은 3가지 Regimen이 권고
F5. ICU 입원환자 (CURB-65 4~5점 이상)
중환자실 입원이 필요한 중증 폐렴은 병합 요법이 원칙
녹농균(Pseudomonas aeruginosa) 감염 위험 여부에 따라 전략이 달라짐.
(1) P.aeruginosa 감염이 의심되지 않는 경우
•
B-lactam + Azithromycin
•
B-lactam + FQ
main | plus |
Amoxicillin/Clavulanate 1.2g IV q 6-8hr
Ampicillin/Sulbactam 3g IV q 6hr
Cefotaxime 2g IV 1 8hr
Ceftriaxone 2g IV q 24hr | Azithromycin 500mg PO/IV q 24hr
Clarithromycin 500mg PO/IV q 12hr |
or | |
Amoxicillin/Clavulanate 1.2g IV q 6-8hr
Ampicillin/Sulbactam 3g IV q 6hr
Cefotaxime 2g IV 1 8hr
Ceftriaxone 2g IV q 24hr | Levofloxacin 750mg IV q 24hr
Moxifloxacin 400mg IV q 24 hr |
(2) Penicillin allergy가 있는 경우
main | plus |
Gemifloxacin 200mg IV q 24hr
Levofloxacin 750mg IV q 24hr
Moxifloxacin 400mg IV q 24 hr | Aztreonam 2g IV q 8hr |
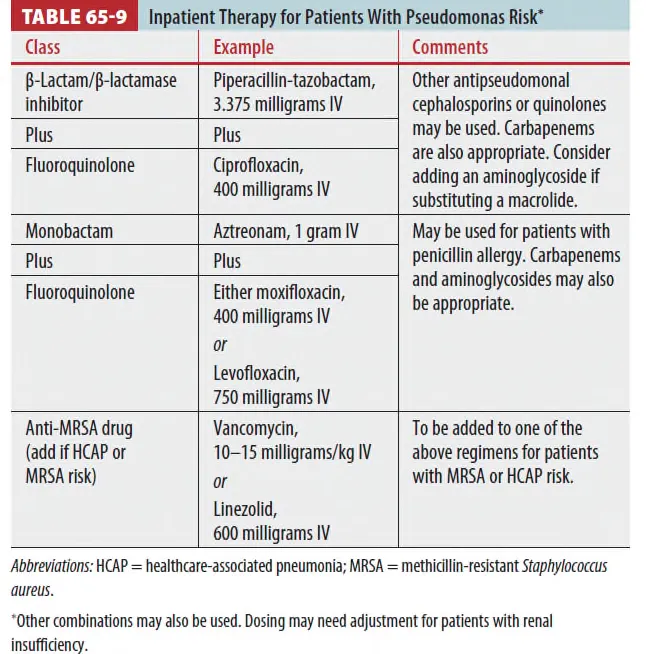
(3) Pseudomonas risk 환자
•
P.aseruginosa의 위험요인
◦
알콜중독
◦
폐의 구조적 질환(bronchiectasis 같은)
◦
반복되는 COPD 급성악화로 Steroid를 자주 투여
◦
최근 3개월 내 항생제 사용력
•
항녹농균 β-lactam + 항녹농균 Quinolone
(cefepime, piperacillin/tazobactam, imipenem, meropenem 중 택 1)
+ (ciprofloxacin, levofloxacin 중 택 1)
•
항녹농균 β-lactam + Aminoglycoside + Azithromycin
•
항녹농균 β-lactam + Aminoglycoside + Quinolone
main | Plus 1 | Plus 2 |
Anti-pneumococcal,
Anti-pseudomonal b-lactam
Cefepime 2g IV 1 12hr
PIP/TAZ 4.5g IV q 6hr
Imipenem 500mg IV q 6hr
Meropenem 1g IV q 8hr | Ciprofloxacin 400mg IV q 12hr
Levofloxacin 750 mg IV q 12hr | |
Anti-pneumococcal,
Anti-pseudomonal b-lactam | Tobramycin 5.1mg/kg IV q 24hr
Amikacin 15mg/kg IV q 24hr | Azithromycin 500mg IV q 24hr |
Anti-pneumococcal,
Anti-pseudomonal b-lactam | Tobramycin 5.1mg/kg IV q 24hr
Amikacin 15mg/kg IV q 24hr | Anti-pneumococcal FQ • Gemifloxacin 200mg IV q 24hr • Levofloxacin 750mg IV q 24hr • Moxifloxacin 400mg IV q 24hr |
(4) Steroids
•
ATS 2025, NEJM 2023년에서 추천
•
초기 bolus: hydrocortisone 100 mg IV 또는 methylprednisolone 40 mg IV
•
이후 중환자실에서: hydrocortisone 200 mg/일(예: 50 mg IV q6h 또는 continuous infusion)으로 4–7일 유지 후, 임상경과에 따라 8–14일까지 점진 감량하는 프로토콜이 대표적입니다.
G. Disposition and follow-up
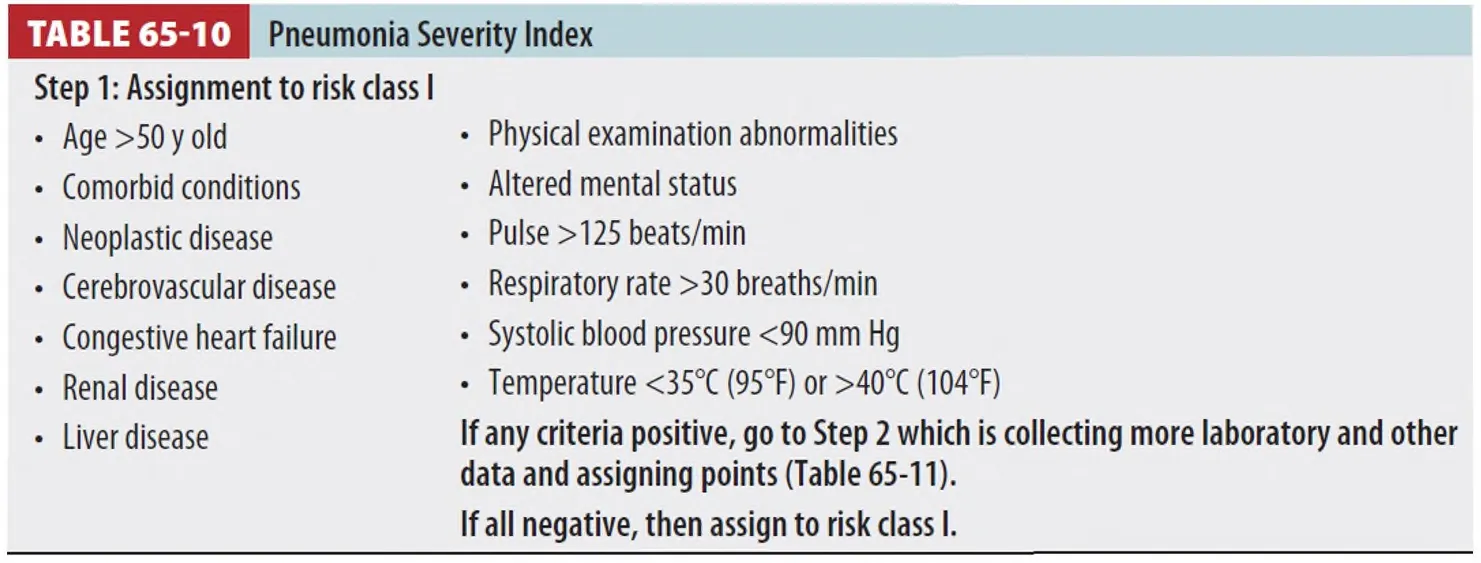
G1. 입원의 결정
은 하기 첨부한 표들을 참조하였을 때, Criteria 중 All negative면 risk class I으로 고
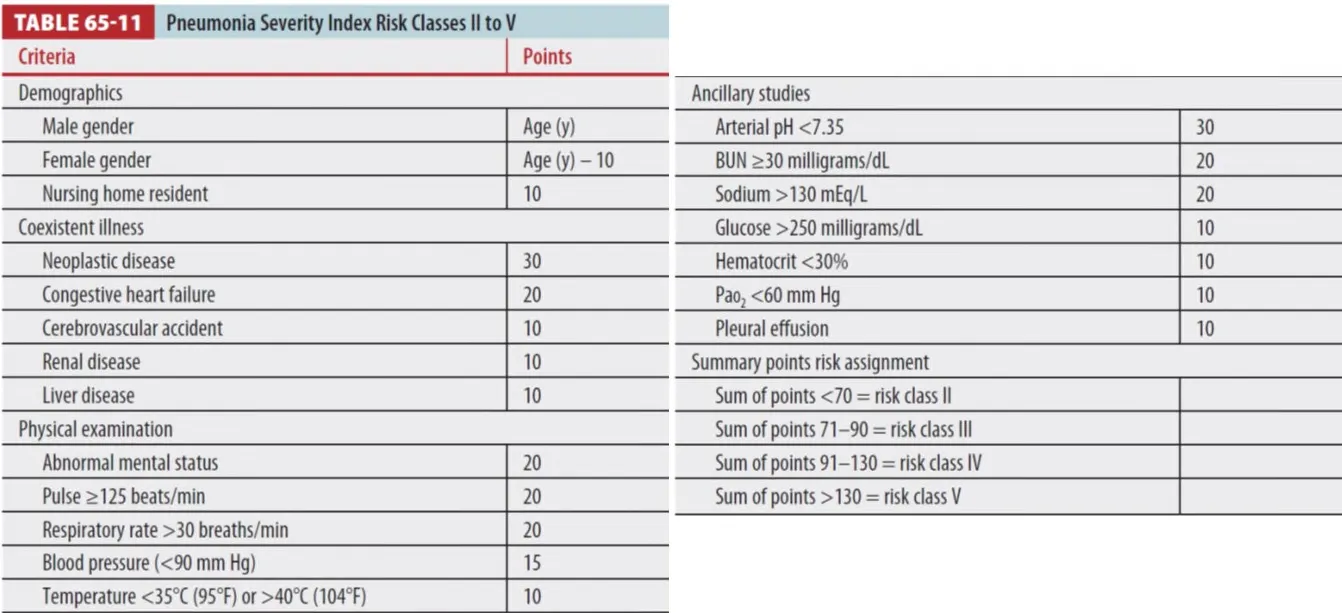
OPD f/u을 결정하게 되며 하나라도 Positive가 있으면 Step 2로 Table 65-11을 참조해 Rick
classification을 시행한다.
(1) Class I~II는 OPD f/u
(2) Class III의 경우에는 Hypoxia의 유무, Social factors, 그리고 oral anti의 섭취 가능 여부 등을 통해
입원 여부를 결정하도록 권고됩니다.
(3) Class IV~V (V의 경우 ICU 고려)는 입원을 결정
G2. CURB-65 rule을 통한 입원 분류법도 있다.
G3. ICU 입원의 또다른 criteria는 다음과 같다.
(1) RR의 급격한 상승 (2) PaO2/Fraction of inspired oxygen ratio≤250
(3) Multilobar infiltrates (4) Confusion
(5) Uremia with a blood urea nitrogen>20mg/dL
(6) Leukopenia (7) Thromobocytopenia
(8) Hypothermia (9) Hyponatremia
(10) Lactic acidosis (11) Asplenia
