

A. Introduction and epidemiology
•
Acute aortic syndrome
◦
Aortic dissection
◦
Penetrating atherosclerotic ulcer
◦
Intramural hematoma (IMH)
◦
Aortic aneurysmal leakage
◦
ruptured abdominal aortic aneurysm
•
Incidence : 연간 2.9~4.7 cases / 100,000 명
•
수술환자에서 mortality rate : 1 year 92%, 5 year 77%, 10 year 57%
•
22%의 환자는 진단 전에 사망
•
Marfan syn.의 M/C cardiovascular complication : aortic root disease와 type A dissection
B. Pathophysiology
•
Acute aortic syn.은 chronic hypertension과 media of aortic wall의 degeneration 을 일으킬 수 있는 요인들로 인해 발생한다.
•
Risk factor : Medial layer를 약하게 하고 , intimal wall stress 를 증가시키는 요소
◦
Bicuspid aortic valve
◦
Marfan syn.
◦
Ehlers-Danlos syn
◦
Aortic dissection의 가족력
◦
만성 코카인 또는 암페타민 사용, 심장 수술 과거력
•
성별에 따른 차이가 있다
◦
Intramural hematoma는 여성에서 더 흔하다 (62%)
◦
여성에서 aortic dissection은 inpatient complication이 흔하며 inhospital mortality 가 높다
B1. Aortic dissection
•
Intima의 손상으로 혈류가 media로 들어와 intima와 adventitial layer 사이가 박리됨
(1) Most common intimal tear site
•
50~65% : Sinotubular junction at the start of the acending aorta
•
20~30%: Just beyond the left subclavian artery at the junction between the acending and descending aorta
(2) Bimodal age distribution
•
위험인자가 있는 젊은 환자
•
>50 세의 만성 고혈압, 허혈성 심장 질환이 있는 환자
(3) Classification
•
Stanford
type A dissection : ascending aorta를 포함한 모든 경우
type B dissection : descending aorta 만 침범
•
Debakey
type 1 dissection : ascending aorta, arch, descending aorta를 동시에 침범
type 2 dissection : ascending aorta만 침범
type 3 dissection : descending aorta만 침범
B2. Aortic intramural hematoma
•
보통 vasa vasorum의 손상으로 생기는 aortic media infarction 의 결과로 생김
•
Penetrating atherosclerotic ulcer에서 진행될 수 있고 스스로 흡수되기도 하고 dissection 으로 진행할 수 있다

C. Clinical features
C1. History
•
전형적으로 갑작스럽고 극심한 흉통, scapula 사이로 방사, 죽을 것 같은 느낌
•
Sharp pain (64%), tearing or ripping pain (50%), syncope (10%)
•
Chest pain 없이 발생하는 경우도 있다 (Asia report 에서는 40%가량)
•
Distal dissection의 경우 등, 옆구리, 복통 등이 생길 수 있음
•
Carotid a. stroke 를 침범한 경우, 전형적인 의 증상을 보이며 spinal cord blood supply 의 가 저해될 경우 paraplegia 발생
•
Aortic root까지 동반된 proximal dissection은 cardiac tamponade 발생 가능
C2. Physical examination
•
대부분은 상대적으로 정상
•
Aortic insufficiency murmur : 32%
•
Radial a. or femoral a. 맥박이 촉지되지 않음 : 15%
•
Hypertension : 49% / Hypotension : 18~25%
•
Aneurysmal dilation으로 구조물 압박
◦
Esophagus, recurrent laryngeal nerve, superior cervical sympathetic ganglion 등 압박
◦
Dysphagia, hoarseness, Horner synd. . 등이 나타날 수 있다
•
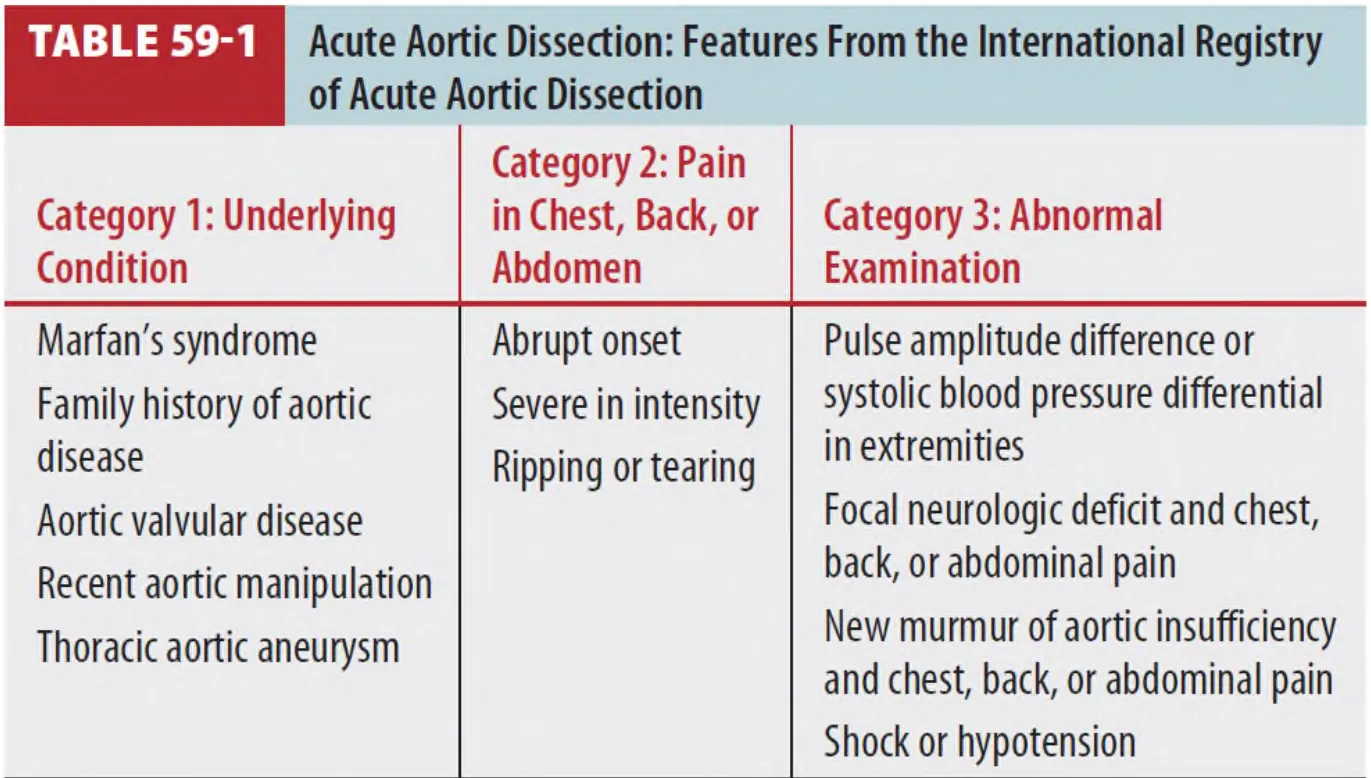
최근 연구를 통해 aortic dissection의 3가지 임상 범주에 따라 12 요소를 분석했고 점수를 매겨 그 점수가 증상이 있는 acute aortic dissection 환자와 유의한 관계가 있음을 확인함.
(the Aortic Dissetion Detection Risk Score ; 각 category별 1점 , 0~3 점 범위)
D. Diagnosis

D1. ECG
•
ACS와 감별 어려움 (Dissection coronary a. blood flow 제한 할 수 있음)
•
19~31%에서만 정상 ECG
(New Q waves, STE 3~4%, STD 15~22%, nonspecific ST, T wave change 41~62%)
D2. Biomarkers
•
D-dimer의 진단적 가치가 연구되었지만 debate 가 있음
•
최근 연구에서 임상적으로 의심되나 the Aortic Dissection Detection Risk Score 의 feature 중 합당한 것이 하나 이하이면서 negative d-dimer(<500ng/ml)인 경우 , aortic dissection 인 경우 의 비율은 매우 낮았다. (0.3%)
•
D-dimer ≥ 0.5 μg/mL 및 연령 조정 D-dimer ≥ [연령(년) × 0.01] μg/mL(최소 0.5 μg/mL)을 양성으로 많이 본다.
측정 시간에 따라 d-dimer 가 차이나지는 않으며, 질환의 심각도가 경증이면 낮게 나타나는 것 같다. (참고문헌)
D3. Imaging
(1) Chest x-ray
•
중요한 단서 제공, 하지만 12~37% 에서 정상소견이므로 배제 목적으로는 사용 불가
•
Widened mediastinum, abnormal aortic contour, pleural effusion, displacement of aortic intimal calcification
•
Deviation of the trachea, mainstream bronchi, or esophagus
(2) CT
•
Modality of choice for diagnosis
•
자세한 구조 및 이상소견 확인 가능 (범위 , end-organ damage, intramural hematoma, ) …
•
Coronary CT angiography (“Triple rule-out" study)
: Coranary a. disease, pulmonary embolism, acute aortic dissection 을 진단할 수 있다
: 진단적 가치, 예후, 의료자원 등에서 더 유리한 것으로 확인되지 않아 추천되지는 않는다.
(3) Other
•
숙련자가 시행하는 TEE는 CT만큼 sensitive & specific 하다
•
MRI는 stable patient 에서 사용
E. Treatment
E1. Antihypertensives
(1) Negative inotropics (Lower BP without increasing the shear force)
(2) β-blocker 를 부적응증이 없는 한 초기에 투여 (COR-1, LOE-B)
•
Short acting이 선호됨 (Propranolol, labetalol, esmolol)
•
Esmolol : Initial bolus 0.1~0.5mg/kg IV over 1min, infusion 0.025~0.2mg/kg/min
•
Labetalol : Initial 10~20mg IV, 이후 repeat dose 20~40mg every 10 min(maximum 300mg)
(3) β -blocker 부적응증이나 intolerence환자
•
Non-dihydropyridine 계 CCB (Vessel보다는 Heart에 주로 작용하는 CCB) 를 사용하여 HR를 조절한다 (COR-2a, LOE-B)
•
Diltiazem (Herben), Verapamil (Isoptin) 을 사용한다.
(4) BP target (COR-1, LOE-C)
•
SBP > 120 mmHg 또는 적절한 end-organ perfusion을 유지할 수 있는 최소한의 혈압 유지
•
맥박수는 60~80 bpm 정도를 목표로 조절
E2. Vasodilator
(1) β-blocker 를 사용에도 혈압 조절 안 되면 추가 (COR-1, LOE-C)
•
IV nicardipine (Perdipine), clevidipine, nitroglycerin, nitroprusside
E3. Pain killer
•
통증조절 위해 pain killer 사용해야 함. (COR-1, LOE-C)
Ⅵ. Disposition and follow up

Malperfusion Tx. Options
AoD : indicates aortic dissection
TEVAR : Thoracic Endovascular Aortic Repair
1.
Surgeon에게 빠른 refer가 꼭 필요하며 emergency open repair가 대부분의 환자에서 TOC이다. 하지만 endovascular repair를 하는 경우가 더 흔하다
2.
중환자실 입원, hemodynamic Tx. & careful monitoring 필요
3.
Acute intermural hematoma, penetrating ulcer의 경우 임상 양상의 명확하지 않아 추후 처치를 결정하는데 이견이 있다.
4.
본원에서는 GS는 infrarenal 만. TS는 Type A만, 그 외는 CV로 입원 (2024.09)
이대서울병원심장혈관 전원 시 카톡으로 보낼 내용
1.
Symptom & onset time
2.
V/S
BP / PR / SpO2 / Mental
Neurologic examination
3.
Vasopressor infusion
4.
C-line, A-line 여부 및 위치
5.
NPO time
6.
키/몸무게/혈액형
7.
과거력/수술력
8.
항혈소판제/항응고제 복용여부
9.
출발예정시간
10.
동행의료진 연락처
Ⅶ. Special considerations
1.
Aortic dissection complicating pregnancy
(1) Rare하며 보통 3rd trimester postpartum period 에 일어난다
(2) Risk factors : Bicuspid aortic valve, connective tissue disorder, HTN, family hx
(3) 진단 시 산부인과, 흉부외과 협진이 필요하다.
