
A. Introduction and epidemiology
1.
Hypothyroidism : Thyroid hormone의 생산이 불충분한 상태 → Metabolism의 저하
2.
고령/백인/여성(10배)에서 많음
3.
모든 연령군에서 Subclinical이 더 많고 고령 여성 4~15%에서 발견됨
4.
현재 치료로 myxedema coma의 사망률은 30~60%
B. Pathophysiology
•
Thyroxine (T4), triiodothyronine (T3)가 thyroid hormone. 혈중 비율은 10:1
•
말초에서 T4가 active T3로 변환되고 T4보다 3~4배 더 potent
•
Half life : T4는 7일, T3는 1일
B1. 일차성 : Thyroid gland 자체의 문제.
(1) Hashimoto’s thyroiditis가 m/c
(2) 수술적 절제술, radioactive ablation, 몇 가지 약물도 원인
•
Drugs: Lithium, α-interferon, interleukin, tyrosine kinase inhibitors.
◦
Amiodarone은 14%까지 hypothyroidism 유발
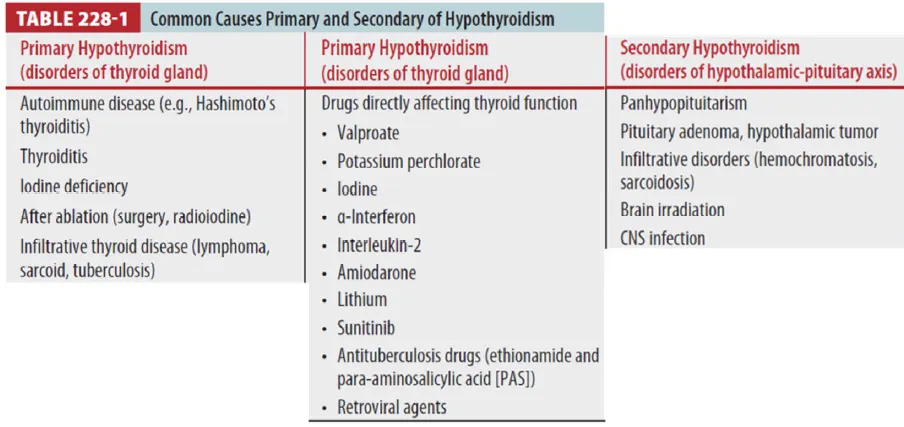
B2. 이차성 : 시상하부-뇌하수체 축의 이상
(1) TSH (pituitary gland), thyrotropin-releasing hormone (hypothalamus) 결핍
(2) Hypothalamic-pituitary axis의 이상으로 인한 중추성 원인
B3. Euthyroid sick syndrome
(1) Low T3 or T4와 normal or low TSH며 임상적으로 euthyroid 환자
(2) 주로 critically ill or severe systemic illness가 있는 환자
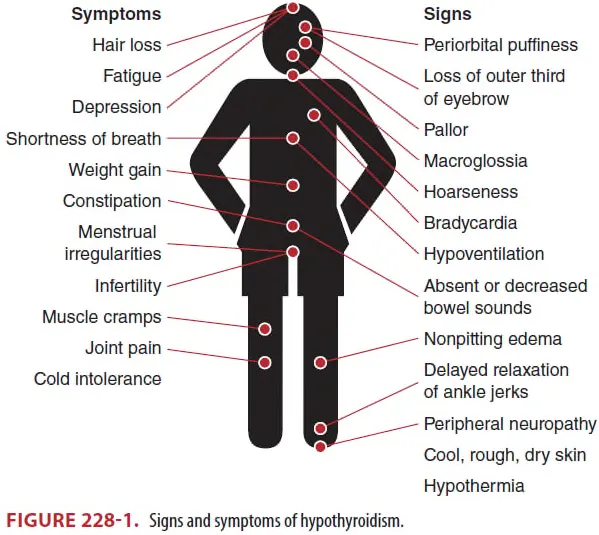
C. Clinical features of hypothyroidism
Additional cardiopulmonary findings
: Angina, Bradycardia, Distant heart sounds from pericardial effusion, Low voltage on ECG,
Pleural effusion, CMP, Hypoventilation
D. Clinical features of myxedema crisis
•
Myxedema crisis (metabolic and multiorgan decompensation)
: Uncorrected hypothyrodism, Mental status changes or coma, and hypothermia (<35.5Ⅳ)
•
Figure 228-1의 증상은 물론 서맥, 저혈압, 저체온, 호흡저하 및 의식 저하/혼수도 동반
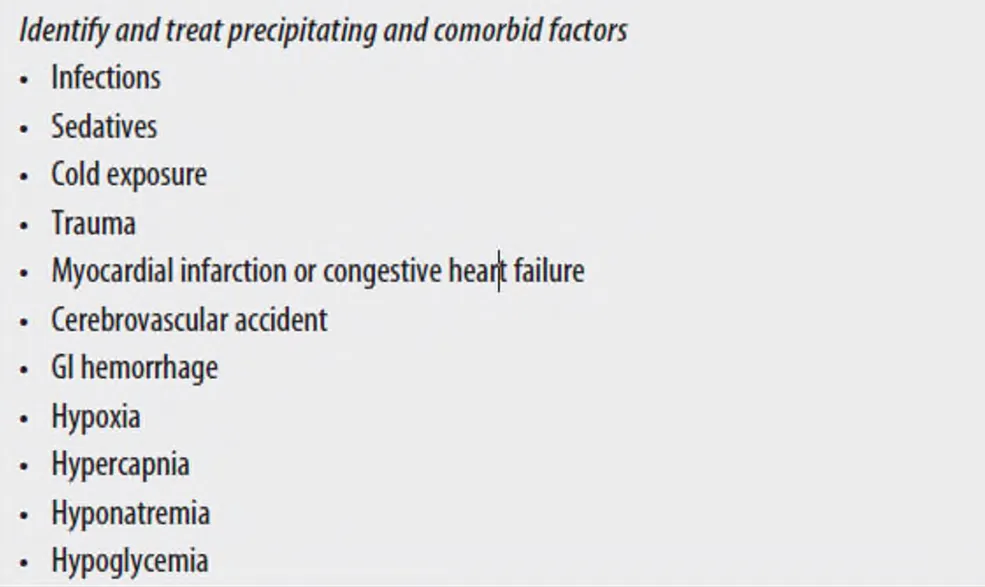
D1. 갑상선 기능 저하 상태에서 myxedema 유발 요인
– 감염, 마취제, 추위 노출, 외상, 심근경색, 심부전, 뇌경색, 위장관 출혈, 수술, 화상, 약물, 호르몬 보충 부재
D2. 저체온
•
정상 체온일 시 underlying infection 감별 필요
•
저체온은 굉장히 흔하여 정상 체온이 오히려 감염 상태일 수 있음.
•
환자의 반은 SBP <100mmHg. 열, 빈맥, 발한이 없지만 감염 상태일 수 있음.
D3. 의식저하
•
호흡 저하로 인한 CO2 narcosis나 저혈당으로 인한 의식 저하 가능성
•
흉수도 흔하고 upper airway edema로 인한 obstruction 가능성
•
마취제 등의 대사가 떨어져 이로 인한 의식 저하 가능성
•
상기 condition에서 저체온은 굉장히 흔하여 정상 체온이 오히려 감염 상태일 수 있음.
E. Diagnosis
•
Hypothyroidism : Lab 결과로 진단
•
Myxedema crisis : 임상적으로 진단.
E1. Laboratory evaluation (TSH, T4, T3, cortisol 치료 전 시행)
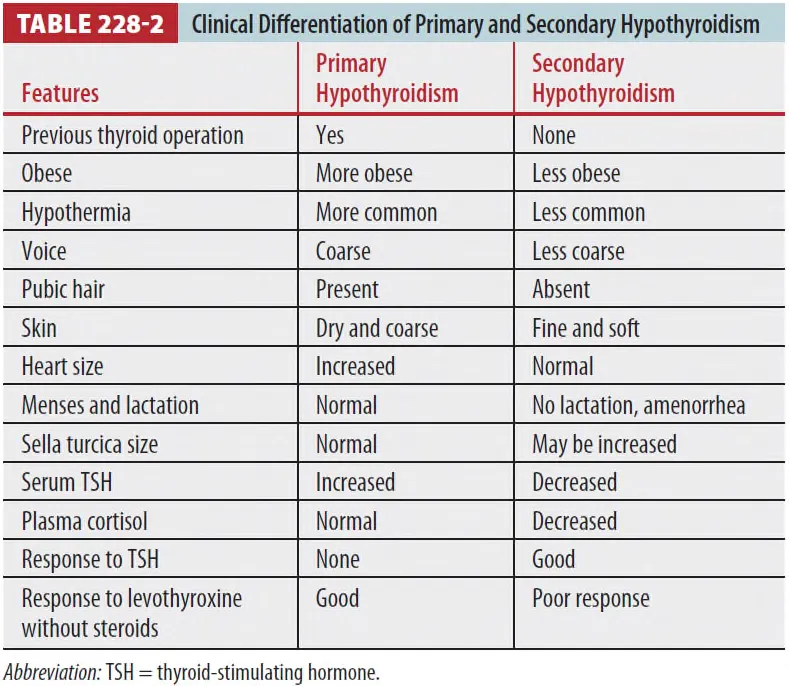
(1) 갑상선 기능검사
•
High TSH + low total or fT4 & T3 → Primary hypothyroidism
•
Low TSH + low total or fT4 & T3 → Secondary hypothyroidism
•
fT4 & T3 assay가 바람직 → Protein binding의 영향을 받지 않기 때문
•
약물상호작용으로 TFT 변해 있을 수 있으나 약물 중단 후 보통 호전됨 (약물 : Tab 228-1)
→ 치료 전 후로 TFT 시행하여야 함
(2) Anemia
•
갑상선 기능 저하로 인한 menorrhagia의 경우 IDA type (microcytic) anemia
(3) Hyponatremia
•
ADH 의 증가 + Impaired free water clearance → Hyponatremia 유발
(4) Hypoglycemia
•
Gluconeogenesis 감소 / insulin clearance 감소 / adrenal insufficiency 혹은 GH 감소
→ Hypoglycemia 유발
(5) ABGA : Hypoxemia, Hypercapnia, MA & RA
(6) ECG : MI / bradytarrhythmias / heart block 확인
(7) CXR : Pneumonia, Pleural effusion, Cardiomegaly 확인
(8) 선행 요인 감별 위한 추가 혈액 검사 시행
F. Treatment of symptomatic hypothyroidism
•
증상 있는 환자에서 확진이 되면 ED에서 oral levothyroxine 시작.
•
Levothyroxine (1.6 mcg/kg, 평균 시작은 50 mcg/d)
: 50세 이상이거나 cardiac disease 있는 경우 half dose로 (12.5~25 mcg/d)
G. Treatment of myxedema crisis
•
Myxedema coma 의심 시 laboratory confirmation을 기다리지 말고 바로 치료 시작!
•
Supportive care + Thyroid hormone replacement + Precipitating factor 확인 & 치료
G1. Supportive care
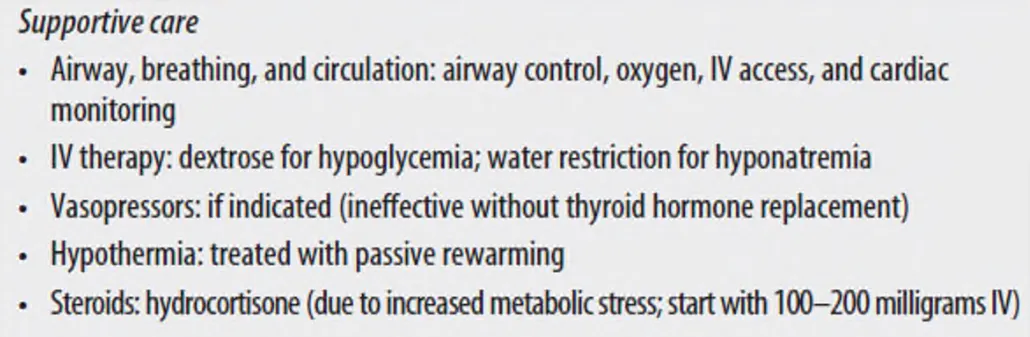
(1) 의식변화 및 호흡부전 → Intubation이 필요한 경우가 많다.
(2) T3 투여 후 부정맥 발생 가능 → Cardiac monitoring 필요함.
(3) 저체온 치료 : Passive rewarming (blanket 사용)
(4) Hypoglycemia → Dextrose containing IV fluid로 교정
(5) Hyponatremia 교정
(6) IV hydrocortisones (특히, 저혈압이 있을 때)
•
100mg IV every 8hrs for first 24hrs
→ Thyroid hormone replacement 전에 첫 dose를 먼저 투여한다.
(7) 경험적 항생제 투여 : Infection이 흔한 precipitating cause이므로.
(8) TSH, T4, T3, cortisol baseline level → 치료 개시 전에 채혈하도록 함.
G2. Thyroid replacement
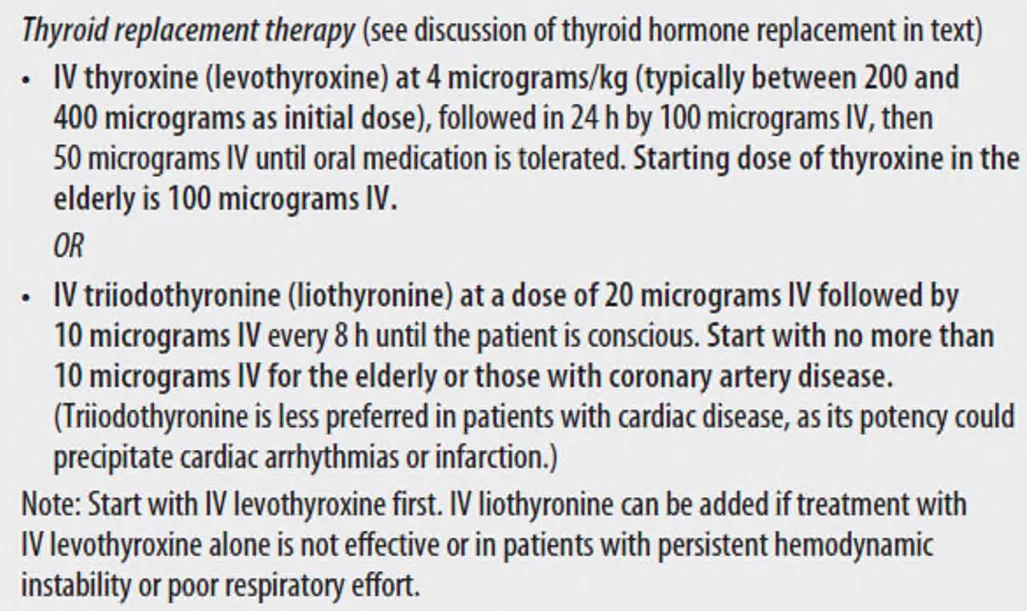
(1) 시작은 반드시 IV route
•
장운동과 GI 흡수가 감소되어 있어서→ 환자 상태 호전(ambulation 가능) 후 PO로 변경
(2) T4 alone, T4 & T3 combination, T3 alone ??
→ 무엇이 좋은지는 아직 잘 모른다.
(3) Severe myxedema coma 환자에서는 T3 투여를 고려
•
이런 환자들에서는 T4에서 T3(active hormone)로 conversion 시키는 능력이 떨어져 있기 때문
•
하지만 T3는 부정맥 유발이 T4보다 흔하므로 compromised myocardial function 있는 환자에서
사용 시 주의가 필요함.
•
빠른 onset of action, but highly fluctuating serum levels
(4) T4 : Smooth, slow, steady onset of action
•
Large therapeutic dose에서 부정맥 및 MI 유발 측면에서 T3 보다 안전함.
G3. Identify and Tx. precipitating and cormorbid factors
H. Dispostion and follow-up
1.
Myxedema coma : High mortality(30~60%) → ICU admission
2.
Poor prognostic factors : Advanced age, bradycardia, persistent hypotension
I. Special populations
I1. Pregnant women
(1) Metabolism의 증가로 thyroid hormone 요구량이 증가됨. (대략 30% 증가)
(2) 산모에서 TFT가 normal이어도 hypothyroidism의 증상이 있는 경우 실제 euthyroid가 아닐 수
있다.
(3) 산모의 subclinical hypthyroidism은 치료 대상임.
(4) Myxedema crisis의 경우 IV levothyroxine이 안전하게 사용 가능.
I2. Elderly / Cardiac patietns
(1) Myxedema crisis 시 예후가 불량. 치료 필요 시 보통 치료 용량의 최고 반으로 시작.
I3. Thyroxine hormone overdose
(1) 24시간 전에는 대부분 증상 발현하지 않음 (T4 → T3 전환 필요)
(2) 적립된 치료법은 없음. 활성탄 투여 가능.
(3) Cholestyramine으로 fecal elimination 증가. Propranolol로 빈맥 및 불안 조절
