
Ⅰ. Diagnosing a Newly discovered Murmur
1.
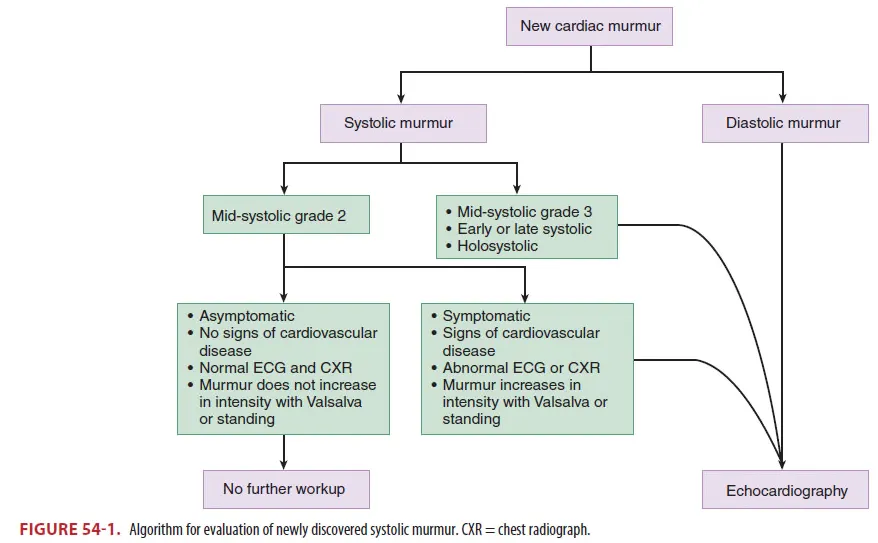
Benign or physiologic murmurs
(1) 다른 심혈관계 질환과 비교할 때 증상이나 이상소견을 야기하지 않음
(2) S1 끝나고 시작하여 S2 전에 끝나는 양상의 soft systolic ejection murmur
(3) Cardiac output을 증가시킬 수 있는 상황에 발생
: Anemia, Sepsis, Volume overload etc.
(4) Underlying trigger에 focus를 두고 검사 및 치료해야 함
2.
Diastolic murmur나 휴식 중 증상을 보이는 new systolic murmur의 경우 질병의 가능성을 고려하여 심초음파를 시행해야함
Ⅱ. Mitral Stenosis
1.
Epidemiology and Pathophysiology
(1) Left ventricle의 정상적인 diastolic filling을 방해한다.
(2) Rheumatic heart disease : 가장 흔한 원인
① 20~40대에 valvular obstruction이 야기됨
② Rheumatic carditis
→ Fusion of valvular commissures, matting of chordae tendineae
→ Eventual calcification and limited mobility of the valve
③ LV로 혈류랑 감소
→ LA pressure↑
→ LA enlargement, pulmonary congestion & hypertension, frequently atrial fibrillation
④ Pulmonary hypertension
→ Pulmonary edema, right-sided heart failure
Bronchial vein rupture까지 일으킬 수 있다.
(3) Mitral annular calcification
① Slow progressive nonrheumatic cause of MS
② 여자, 노인, 고혈압. 만성 신부전
③ 천천히 진행하여 mitral valve stenosis를 유발하므로 심각한 증상을 유발하진 않음
2.
Clinical Features
(1) Exertional dyspnea
: M/C sx.으로 cardiac demand가 증가하는 infection, anemia와 같은 상황에 의해 악화될 수 있다
(2) Hemoptysis (rare)/ Orthopnea / Premature atrial contractions / Systemic emboli d/t A.fib
(3) Severe obstruction : Left or right side heart failure로 야기될 수 있는 증상들
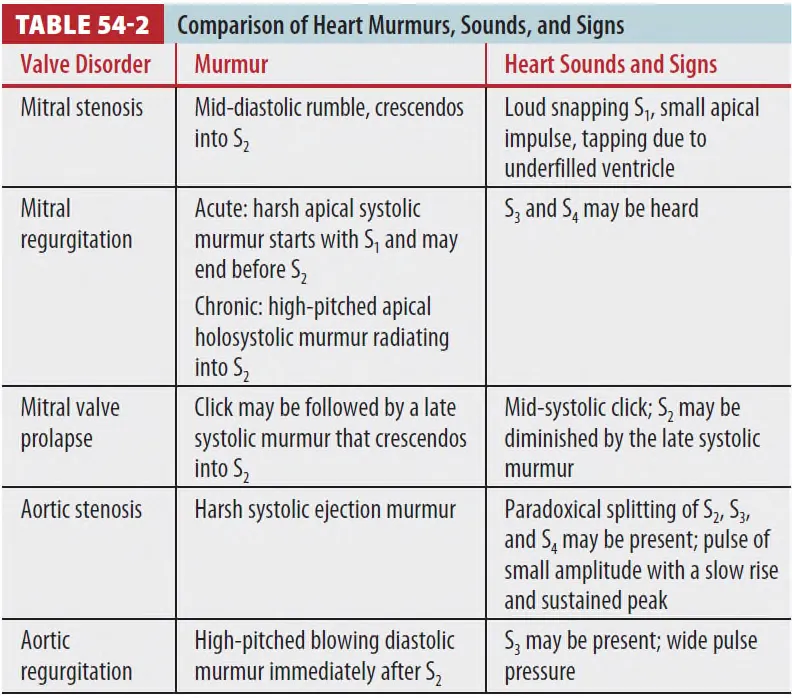
(4) Mid-diastolic rumbling murmur with crescendo toward S2
(5) Atrial fibrillation
① Presystolic accentuation
② S1 이 loud하게 들림
③ Left ventricle의 filling 이 잘 안되므로 apical impulse는 작아짐
3.
Diagnosis
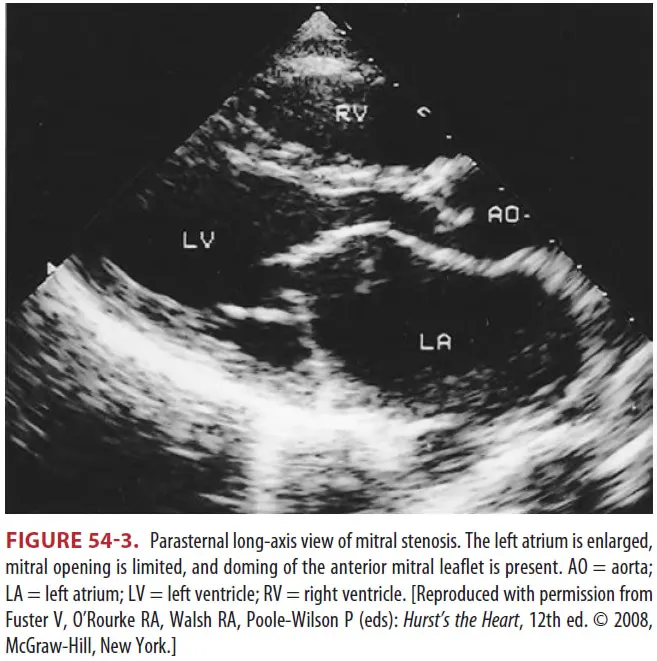
(1) 초음파로 진단
① Transesophageal echocardiography (Fig 54-3)
② Mitral valve regurgitation degree, left atrial thrombus 존재 평가
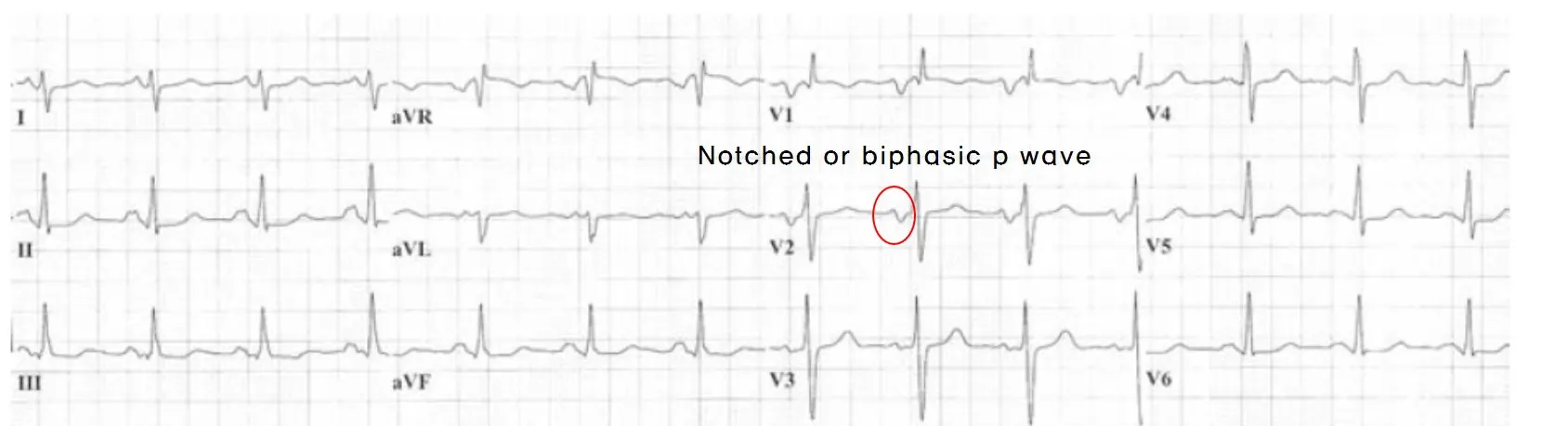
(2) 심전도
① 심방세동 (가장 흔한 합병증)
② Notched or biphasic p wave (Fig 54-2)
③ Rt. axis deviation

(3) Chest X ray
① Left heart border의 straightening
② Left atrial enlargement → Eventual pulmonary congestion occurs
4.
Treatment
•
증상 완화, A. fib 치료, 항응고 치료
(1) 증상이 있거나 A. fib이 있는 환자
① β-blocekr, CCB 사용 → Heart rate control을 통한 이득을 볼 수 있다.
(2) Anticoagulation treatment indication
① Left atrial diameter >55mm, A. fib patients, Left atrial thrombus
② Systemic emboli의 기왕력이 있는 자
(3) MS-induced pulmonary edema로 인한 hemoptysis
① 수혈, 응급 기관지 내시경, 흉부외과 의뢰
(4) 증상 있는 MS는 mechanical intervention 필요
① 폐부종이 심해지기 전에 해야 한다.
② Balloon valvotomy / Valve repair / Valve replacement
Ⅲ. Mitral Regurgitation
1.
Epidemiology and Pathophysiology
(1) Systole phase에서 mitral valve dysfunction으로 인하여 LV에서 LA로 blood flow가
regurgitation
(2) 원인
① Fibroelastic deficiency syndrome (m/c)
② Mitral valve prolapse (young patient)
③ Papillary muscle displacement
④ Valve dysfunction
(3) Chronic MR : LA 확장으로 서서히 진행
(4) Acute MR : Papillary muscle or chordae tendineae rupture from MI
(5) Valve leaflet perforation from infective endocarditis, blunt thoracic trauma와 spontaneous
chordae tendineae rupture에 의해 급격하게 발생
2.
Clinical Features
(1) Acute MR
① Severe dyspnea, Tachycardia, Pulmonary edema
② Cardiogenic shock나 cardiac arrest로 급속하게 진행
③ 호흡곤란으로 협심증을 놓칠 수 있음
(2) Chronic MR
① Exertional dyspnea, A. fib (Can be tolerated for years without sx.)
3.
Diagnosis
(1) Acute MR
① 새로 발생한 pulmonary edema & near-normal heart size on chest radiograph에서는
의심해야 함
② EKG : Inferior or anterior wall에서 ischemic sign이 있는지 확인.
(2) Chronic MR
① EKG : LA enlargement, LV hypertrophy
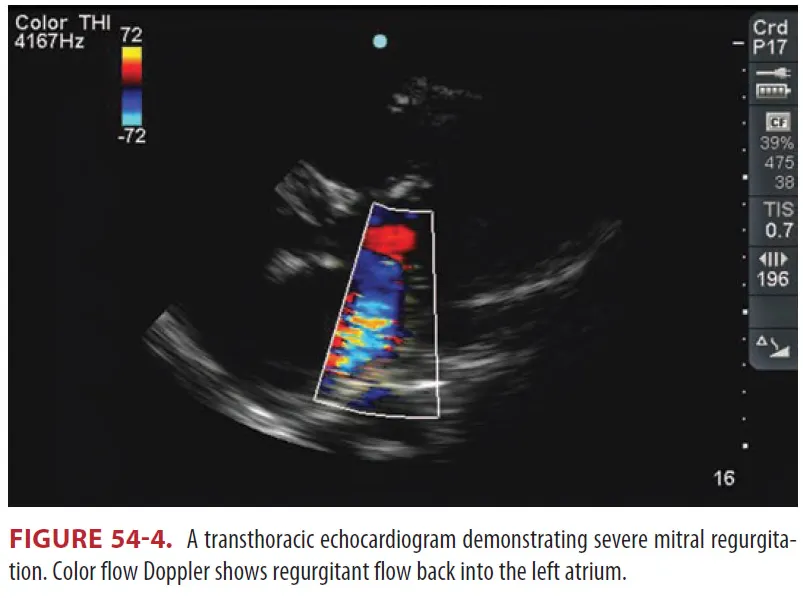
(3) Transthoracic echocardiography → Transthoracic echocardiography or cardiac MRI
(4) Exercise stress echocardiography
4.
Treatment
(1) Papillary muscle rupture에 의한 acute MR은 emergency surgery
(2) Nitrate : Afterload를 줄여줌
(3) Inotropic therapy를 할 때 Dobutamine 함께 사용
(4) Aortic balloon counterpulsation
: Regurgitant volume과 left ventricular filling pressure를 줄여줌
(5) ED에서는 start therapy with oxygen and positive-pressure ventilation for respiratory failure
(6) AMI에 의한 severe mitral regurgitation은 emergent revascularization이 필요
(7) Endocarditis에 의한 MVP는 antibiotics therapy가 필요
(8) Chronic MR
① β-blocker, CCB to control a.fib RVR
② Start anticoagulation to avoid embolization
Ⅳ. Mitral valve Prolapse
1.
유전질환 중에 connective tissue protein의 defect에 의한 판막의 myxomatous degeneration으로
인하여 one or both leaflets의 left atrium으로 systolic billowing 되는 것을 말함
2.
선진국의 가장 흔한 판막 질환 : 인구의 2.4% / 대부분의 환자는 무증상
3.
비전형적 흉통, 두근거림, 피로감, 불안감, 운동과 무관한 호흡곤란
4.
Scoliosis, pectus excavatum, 체중저하와 연관됨
5.
Physical exam
(1) Mild-systolic click
(2) Preload decreased (valsalva, standing) → Early diastole에서 click
(3) Preload ↑ (Squatting) , Afterload ↑(Hand grip) → Systolic click이 systole 후반에 발생
6.
치료
(1) Palpitation이 있을 때는 β-blocker가 도움
(2) Anti-thrombotic therapy는 routine으로 추천되지 않음
(3) MR이 있은 MVP는 심내막염 예방이 필요
(4) ED 내에서 treatment가 필요한 경우는 드물다.
Ⅴ. Aortic Stenosis
1.
Epidemiology and Pathophysiology
(1) Left ventricular outflow를 감소시킨다.
(2) 위험인자 : Increasing age / Hypertension / Smoking / Elevated cholesterol / Diabetes
(3) 가장 흔한 원인은 degenerative calcification
(4) Rheumatic heart disease가 주된 원인임
(5) 젊은 사람은 bicuspid aortic valve, 다른 선천성 심질환 등이 있는 경우가 많다
(6) 주된 clinical course
Long asymptomatic period → LVH가 EF가 preserve
→ Ventricular hypertrophy가 결국 diastolic filling의 impairment를 야기
→ Myocardial oxygen demand를 상승
→ Aortic valve obstruction worsen, cardiac output diminishes
→ Systemic, coronary blood flow의 장애 야기
2.
Clinical Features
(1) 고전적 삼징후 : Dyspnea, Chest pain, Syncope
(2) Aortic valve area <1.0cm2에도 aymptomatic, but 한 번 증상 발현 시 mortality는 증가한다
(3) 심방세동은 드물지만, 임상 경과 악화와 연관됨
(4) Late peaking systolic murmur at the right second intercostal space,
radiating to the carotids
(5) Pulsus parvus et tardus
: 한 개 또는 paradoxically split S2, S4 gallop 후 upstroke 지연되면서 carotid pulse가 사라진다
3.
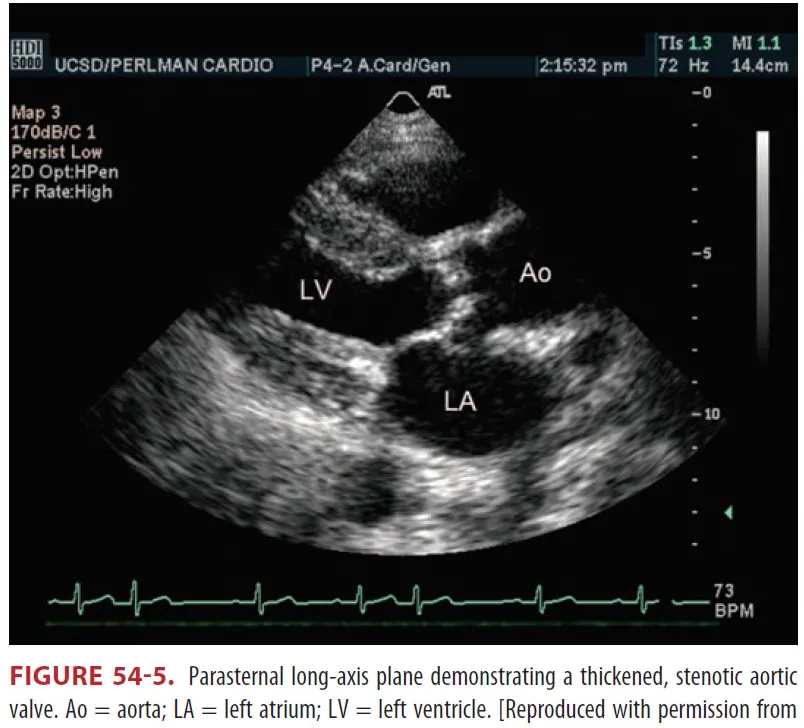
Diagnosis
(1) 심초음파
(2) ECG와 Chest x-ray는 민감도와 특이도가 부족
① ECG : 10%, RBBB
4.
Treatment
(1) 폐부종에 대한 치료 : 산소 및 양압 환기
(2) Newly symptomatic aortic stenosis의 모든 환자는 수술을 받아야 한다
수술 받지 않으면 1년 안에 40~50% 사망
(3) Nitrates, vasodilators, diuretics의 사용은 preload와 afterload에 영향을 미쳐 저혈압을 유발함으로
신중하게 사용해야 한다.
(4) New onset A. fib 있는 경우 may require cardioversion to maintain cardiac output
Ⅵ. Aortic Regurgitation
1.
Epidemiology and Pathophysiology
(1) Valve leaflets 이 완전히 닫히지 않아 blood flow가 diastole phase에 aorta로부터 LV로 생김
(2) LV pressure ↑, LV dilatation and hypertrophy
(3) Wide pulse pressure
: Diastole 동안의 빠른 pressure drop으로 인하여 stroke volume이 증가하여 발생함
(4) Valvular leaflet problems
① Bicuspid aortic valves ② Infective endocarditis ③ Rheumatic dz.
(5) Non-valvular leaflet problems
① Aortic dissection ② Marfan’s syndrome ③ Aortitis
2. Clinical Features
(1) Acute AR
① Dyspnea와 pulmonary edema가 가장 흔한 증상
② Cardiac output이 유지되는 경우에는 tachycardia가 나타나지만
심한 경우 cardiogenic shock, cardidac arrest를 일으킬 수 있다.
(2) Sudden-onset ripping or tearing interscapular pain은 aortic dissection을 의심
(3) Fever or a history of IV drug abuse는 endocarditis을 의심
(4) 이완기 심잡음이 들릴 수 있다.
① High pitched blowing diastolic murmur at 2nd, 3rd intercostal space)
② 그러나 급성의 경우 심잡음이 작거나 짧아서 들리지 않음
(5) Water hammer pulse : stroke volume 증가로 인해 빨리 pulse가 올라갔다가 내려감
(6) “to and fro” femoral murmur (Duroziez's sign) : Femoral artery의 systolic, diastolic bruit
(7) de Musset sign : 심박에 따라 머리가 위아래로 움직임
(8) Quincke sign : 손톱 압박했을 때, 손톱 아래 빨간 부분과 흰 부분 경계선(unguis)이 박동하는 현상
(9) Chronic AR
① Exertional dyspnea ② Fatigue ③ Chest pain
④ Palpitations ⑤ Left ventricular failure 증상
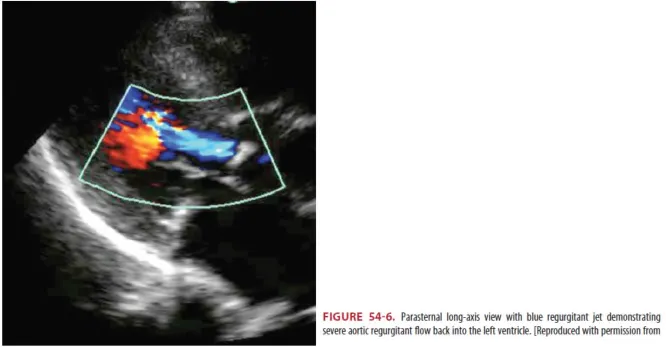
3. Diagnosis
(1) 심초음파
(2) Chest X-ray : Pulmonary edema, Widened mediastinum (Aortic dissection)
(3) ECG : Sinus tachycardia, nonspecific
(4) Aortic dissection이나 infective endocarditis을 고려해야 함
4.
Treatment
(1) Acute AR
① 즉각적인 수술이 필요
② Pulmonary edema treatment : Oxygen & Intubation
③ Nitroprusside와 dobutamine/dopamine 함께 사용
: forward flow를 늘리고 left ventricular end-diastolic pressure를 줄여준다
④ Diuretics, nitrates는 효과가 약하다
⑤ Aortic dissection에서 β-blocker를 사용하지만 AR에서 생기는 보상성 빈맥 방해하므로 피해야 함
⑥ IABP도 금기 : regurgitation flow를 악화시킨다
⑦ Endocarditis : Antibiotics - 수술적 치료 즉각적으로 하지 말고 고려
(2) Chronic AR
① Vasodilators(ACEi, CCB)
② Aortic valve replacement : 증상이 있고, EF가 낮고, 심한 LV dilatation 있는 경우 고려
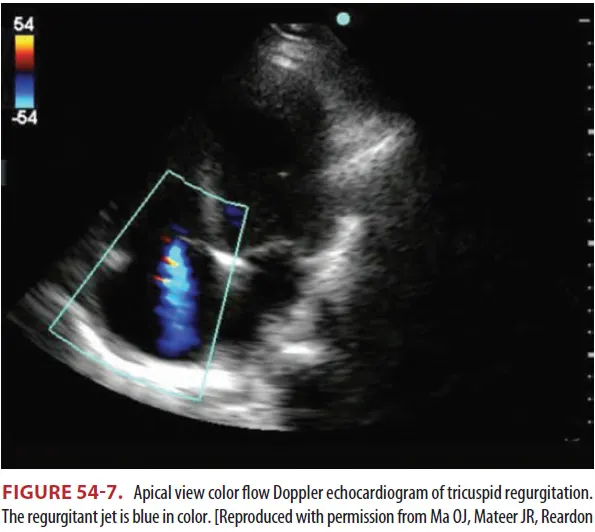
Ⅶ. Right-side Valvular Heart Disease
1.
Epidemiology and Pathophysiology
(1) Pathologic tricuspid regurgitation
① 폐동맥 고혈압, 만성 폐쇄성 폐질환, 폐동맥 혈전증, 심방 중격 결손 같은 우심실 압력의 증가
상황에서 발생
② 용적 과부화를 유발하는 상황에서 발생
(2) Tricuspid stenosis : Regurgitation에 의해 유발 가능, rare
(3) Pulmonic valve : Congenital cause
(4) Acute onset of symptomatic tricuspid disease : Endocarditis. S. aureus
2.
Clinical Features
(1) Symptom of Rt Heart failure
① Jugular venous distension ② Peripheral edema ③ Hepatomegaly
④ Splenomegaly ⑤ Ascites ⑥ Exertional dyspnea
(2) Physical exam
① TR
: Soft, bloing, olosystolic murmur at the lower left sternal border
② TS
: Rumbling crescendo-decrescendo diastolic murmur before S1 at the lower left sternal
border
(3) PS
① Extertional dyspnea, syncope, chest pain, Rt Heart failure의 symptom
② Harsh systolic murmur at the left second intercostal space
(4) PR
A high-pitched and blowing diastolic murmur at the ① left second and third intercostal
spaces
3. Diagnosis
(1) 심초음파 : 진단적 Tool, 경식도 초음파가 민감도 더 높다.
(2) Chest X ray & ECG : nonspecific
4.
Treatment
(1) Undelying cause treatment
(2) Diuretics
① Ascites. edema에 대해 치료로 사용할 수 있다.
② 전해질 불균형, volume depletion 등을 유발할 수 있으므로 조심히 사용
Ⅷ. Prosthetic Valve Disease
1.
Epidemiology and Pathophysiology
(1) Mehcanical valve 및 bioprosthetic valve로 나뉨.
(2) Mechanical valve
① 내구성이 좋다.
② Thromboembolism의 위험성이 증가하여, 오랜 기간 anticoagulation이 필요하다. (INR : 2.5~3.5)
(3) Bioprosthetic valve
① Thromboembolism의 위험성은 낮다.
② 판막부전이나 재수술의 가능성이 있음 (INR : 2.0 ~ 3.0)
(4) 3개월 동안 증가 : MVR이 AVR 보다 자주 발생
(5) Prosthetic valve endocarditis의 원인균
① 수술 후 1년 내 : S. epidermidis, S. aureus.
② 후기에는 원래 판막과 유사 : Streptococcus viridans
2. Clinical Features
(1) 판막 치환술 후에도 많은 환자들은 증상이 지속 된다
(2) 판막의 혈전생성은 여러 장기에 영향을 줄 수 있다
(3) Major embolic event – Stroke / Mesenteric infarction / Sudden death
(4) Anticoagulation 치료는 중증 출혈의 원인이 되기도 한다
(5) 급격한 respiratory distress, pulmonary edema, cardiogenic shock은 mechanical valve failure,
bioprosthesis tearing, valve의 large clot obstruction, preventing closure와 연관이 있다
3. Reversal of anticoagulation with prosthetic valves
(1) Mechanical valves : mitral - INR 2.5~3.5 , bileaflet - INR 2.0~3.0
(2) Aspirin : Recommend for all patients with prosthetic valves (Mechanical, Bioprosthetic)
(3) INR 5~10 : Warfarin 끊고 1.0~2.5mg oral vitamin K를 준다.
(4) 심각한 bleeding
① FFP, prothrombin complex concentrate를 준다.
② Parenteral, high dose vitamin K 는 over correction을 피하기 위해 주지 않는다.
