
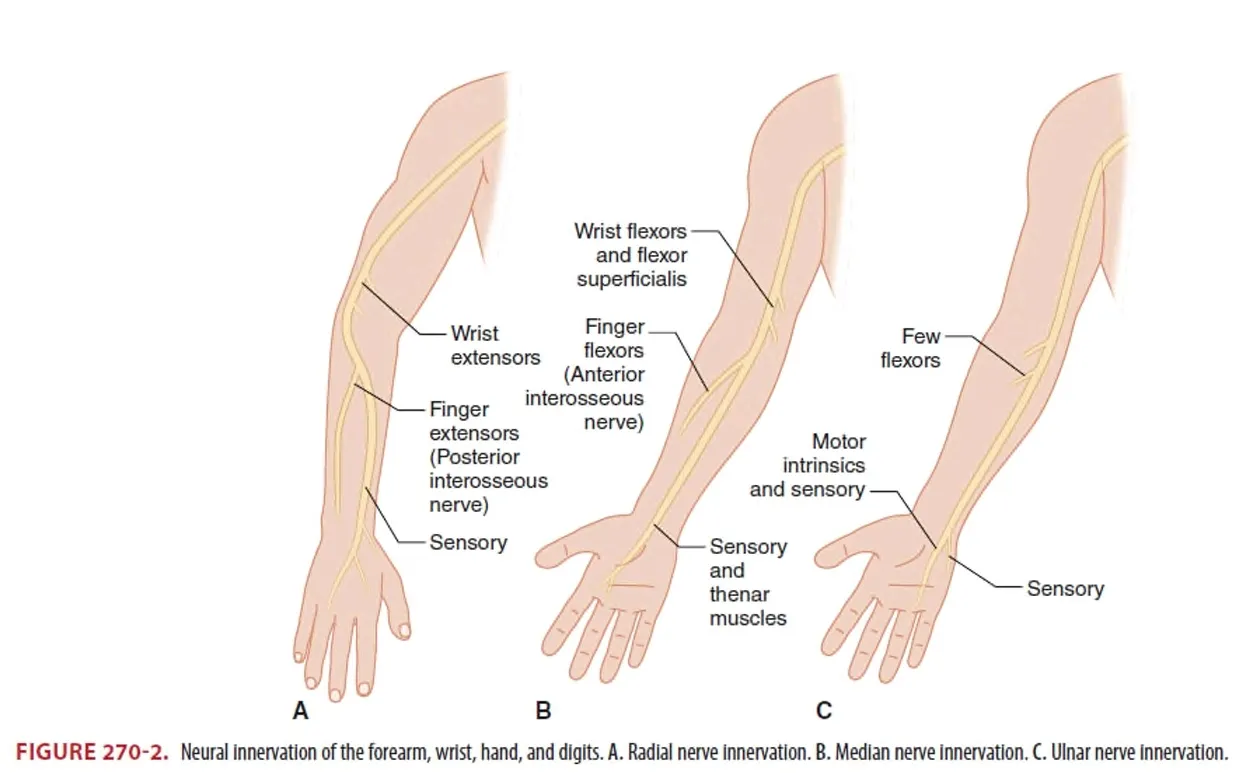
A. Anatomy & Physical Examintation
★ 매우 중요한 표로 각각의 신경에 대한 function test는 숙지하고 있어야 합니다.


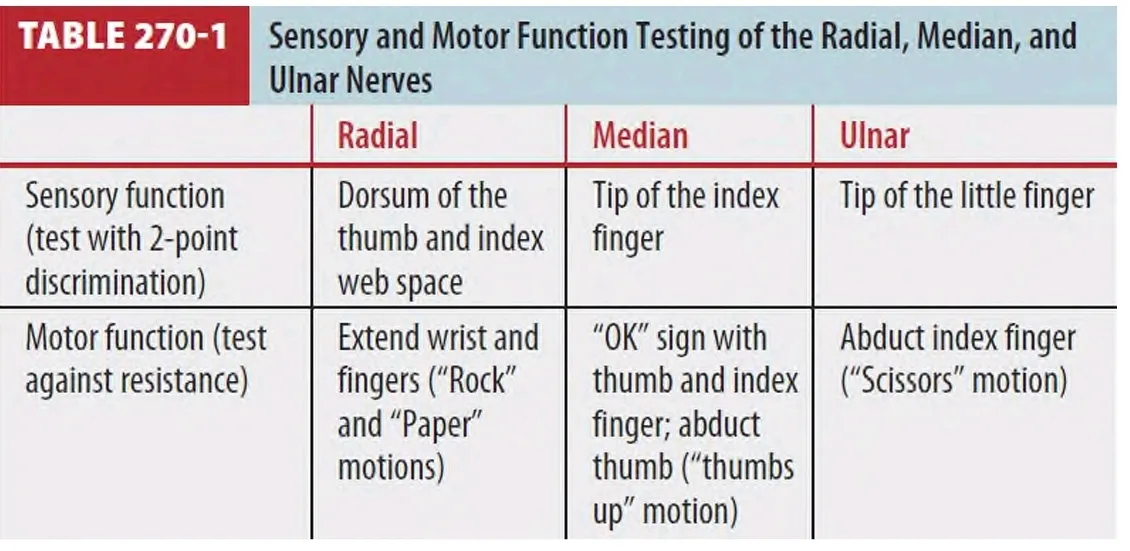
A1. Radial n.
(1) Motor : Wrist extension, Finger & Thumb extension
(2) Sensor : Over the dorsal aspect of the hand from the thumb to the radial half of the ring finger
A2. Median n.
(1) Motor : Wrist flexion, Finger & Thumb flexion
(2) Sensor : The volar surface of the hanfrom the thumb to the radial half of the ring finger, including the dorsal tips of the thumb, index, middle fingers
A3. Ulnar n.
(1) Motor : Finger abduction
(2) Sensor : Little finger and ulnar half of the ring finger

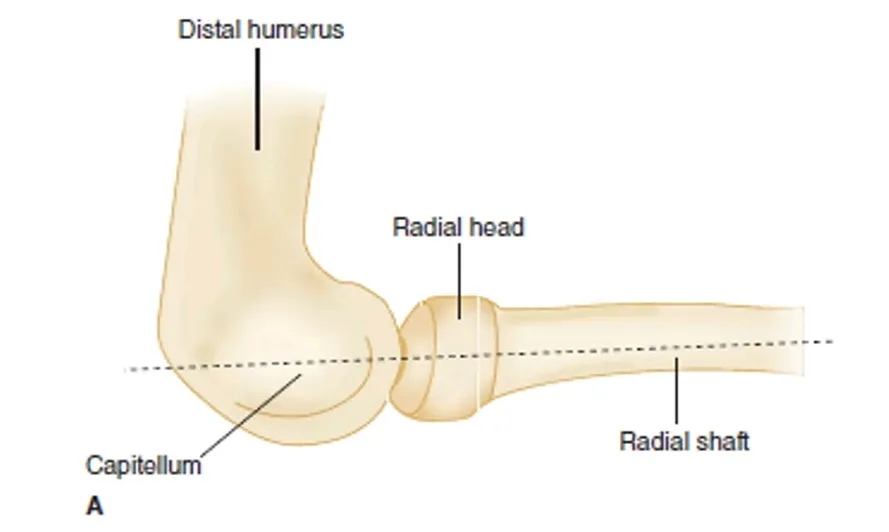
B. Diagnosis
•
Lateral view에서 radial shaft의 중앙을 관통하는 선을 그렸을 때 radial head와 capitellum을 양분하는데 이러한 관계가 소실되었을 때 radius의 fracture나 dislocation일 가능성이 높음.
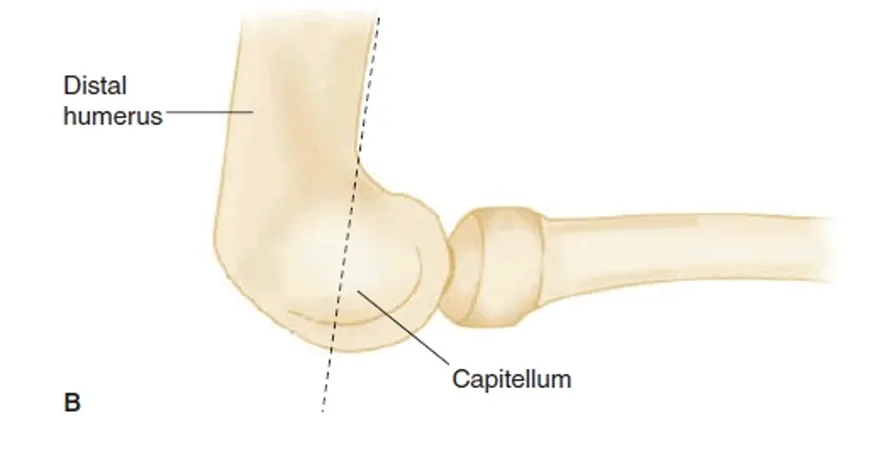
•
Humerus의 전방 경계를 따라 내린 선이 capitellum의 후방 2/3지점을 통과하는데 이러한 관계가 소실 시 distal humerus fx. (성인) 혹은 supracondylar fx. (소아)일 가능성을 시사함.
C. Soft tissue injuries
C1. Biceps tendon rupture
•
거의 대부분 proximal long head를 involve
•
Anterior shoulder pain, tenderness, swelling, ecchymosis (biceps 따라서)
•
Elbow 굴곡 시 biceps muscle이 distally retraction되면서 midarm에 ball 형성
(1) Biceps squeeze test (Thompson test와 비슷)
① 환자가 앉고 forearm을 60~80도 flexion시킨 상태
② 검사자의 한 손을 biceps brachii의 muscle belly에,
다른 한 손을 myotendinous junction에 놓고 양손으로 쥐어짠다
③ Forearm이 supination (음성, 정상) ⇒ biceps가 intact함을 나타낸다.
④ Supination 안 되면 (양성, 이상) ⇒ distal biceps brachii rupture로 간주된다.
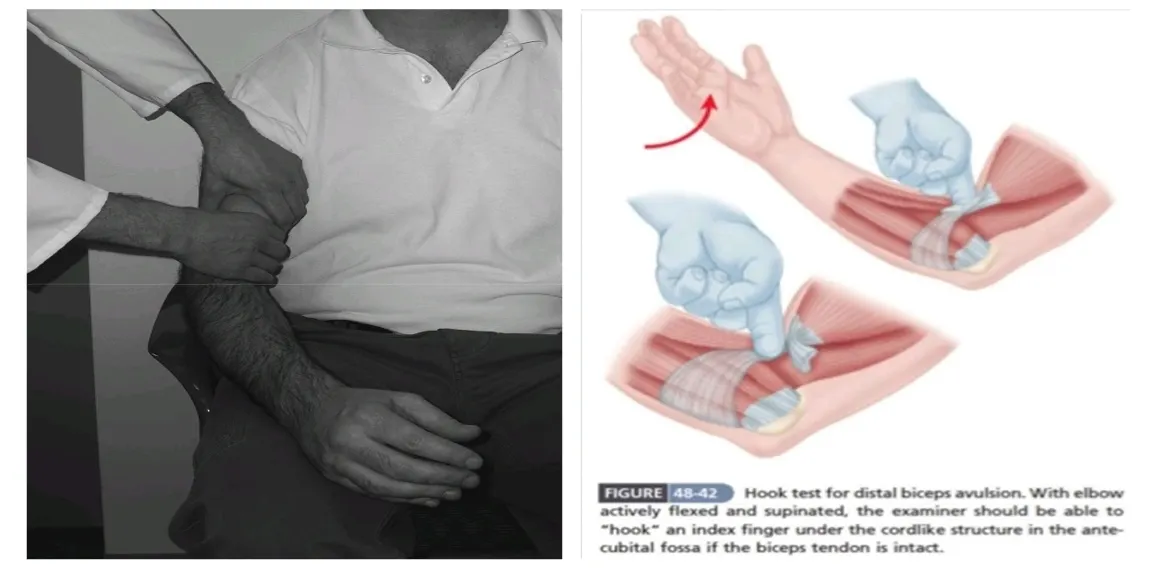
(2) Hook test
① 환자의 elbow를 90도 flexion & active supination 시킨다
② Biceps tendon이 intact하다면
: 검사자는 antecubital fossa의 distal biceps tendon 아래로 index finger를 걸 수 있다.
C2. Triceps tendon rupture
•
Rare, 대부분 distally
•
Posterior elbow pain, elbow swelling, tenderness
•
Complete rupture : elbow extension이 안됨.
(1) Modified Thompson test
•
Arm을 받친 채, forearm이 relaxed position으로 90도 flexion하여 hanging돼 있도록 자세를 취한다.
•
Complete rupture가 있지 않다면, triceps muscle을 쥐어짤 때 forearm이 extension된다.
C3. Lateral epicondylitis (Tennis elbow)
(1) Tennis elbow, overuse syndrome
(2) Lateral epicondyle tenderness, wrist, digit extension, forearm supination시 제한, 통증
C4. Medial epicondylitis
(1) Golfers elbow
(2) Wrist, digit flexion과 forearm pronation 시 제한, 통증
D. Elbow
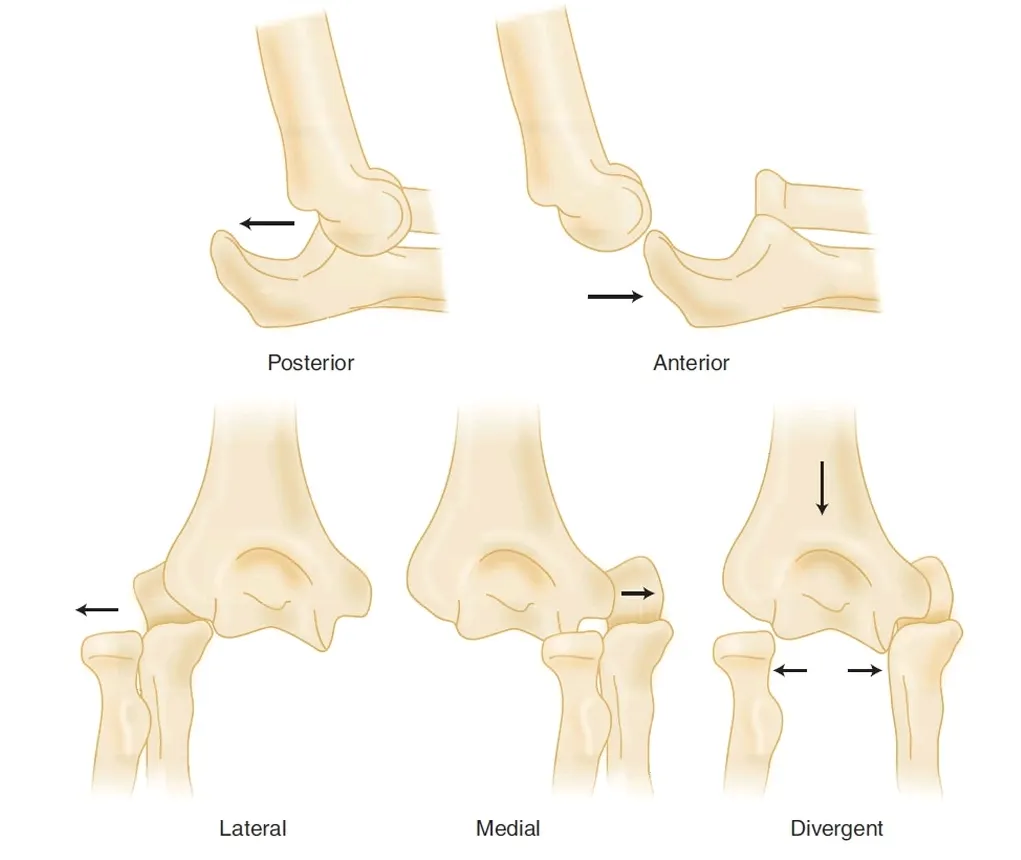
D1. Elbow dislocation
•
Posterolateral (m/c : 90%)
(1) Complication
•
신경손상 : 8~21%, Ulnar n. 가 m/c
•
혈관손상 : 5~13%, Brachial a. 가 m/c
(2) 치료
•
Reduction 후 splint (axilla~finger base까지) 90°flexion
•
석고는 하지 않고, 1~2주 후 Early ROM program (Table 270-3)
Irreducible dislocation / Neurovascular compromise / Postreduction instability Associated fracture / Open dislocation → Emergency OS consultation

(3) Terrible triad injury
•
Unstable joint (Elbow dislocation + Fx. of radial head and coronoid)
→ Initial reduction 후 surgical repair가 필요함.
D2. Fracture about the elbow
•
Abnormal fat pad on elbow
: 정상에서 posterior fat pad는 보이지 않으며 anterior fat pad는 정상적으로 thin lucent stripe으로 보일 수 있다 : Elbow injury 발생 시 posterior fat pad는 후방으로 이동하여 posterior fat pad를 보이고 anterior fat pad는 prominent 하게 되어 sail sign을 보인다.
: 이러한 Abnormal fat pad는 joint effusion과 같은 nontraumatic 조건에서도 보일 수도 있다.

(1) Distal humerous fractures
•
Brachial artery 주의
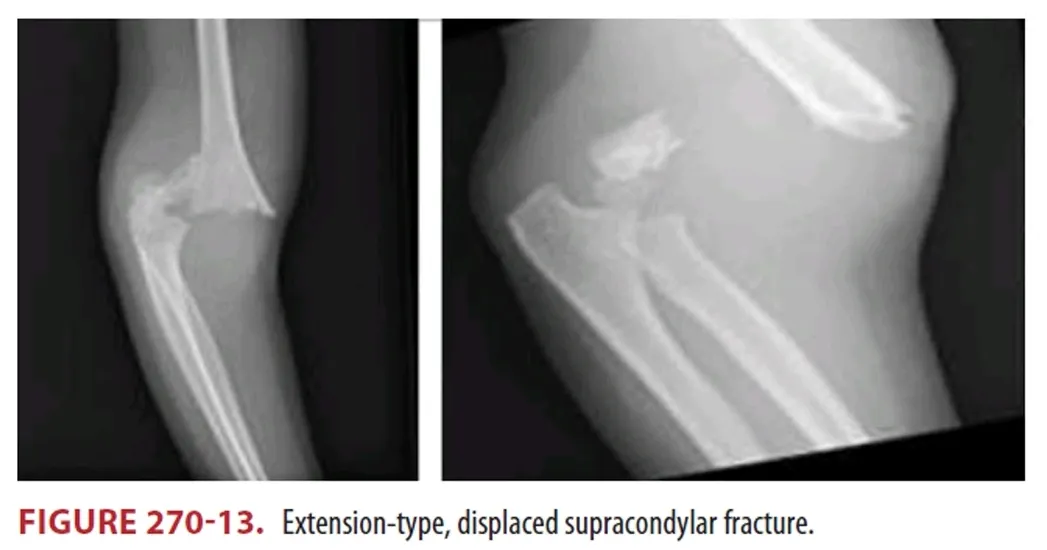
(2) Supracondylar fractures
•
Extension-type (m/c 95%)
: 비전위골절의 일부에서는 골절선이 보이지 않고 "fat-pad sign" 만 골절의 유일한 증거가 될 수 있다.
•
Flexion-type (rare 5%)
: 수상 기전 - Direct force against flexed elbow : 개방성 골절이 많다.
•
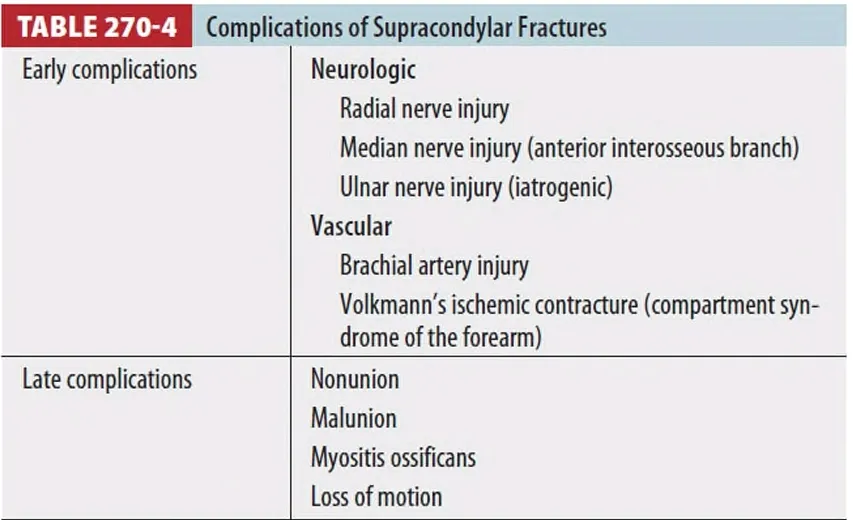
Complication of supracondylar fractures
◦
급성 혈관, 신경 손상을 항상 염두
▪
Posteromedial displacement - Radial n. injury
▪
Posterolateral displacement - Median n. injury
▪
Supracondylar fx. - Anterior interosseous n. injury
median n.의 branch → OK sign이 되지 않음. 순수운동신경이므로, 감각은 정상
FPL, FDP, Pronator quadratus에 innervation
◦
Volkmann's ischemic contracture (Forearm의 compartment syndrome)
▪
Postischemic swelling → pr. ↑, capillary blood perfusion ↓
: 손을 펴려고 하지 않음 : 강제로 손가락 extension 시 pain 호소, forearm tenderness
: 치료 - Supracondylar fx. + Radial pulse 없을 때
→ Closed reduction & Percutaneous pinning
→ Pulse X, Ischemia sign O : Fasciotomy and/or bracheal a. exploration
→ Pulse O, Ischemia sign X : Closed observation : Observation for 24~36h followed by arteriography & surgery if indicated : Immediate surgery
(3) Intercondylar fractures
① Condylar fragment가 분리되어 있으며 소아보다 성인에 흔함.
② CT 검사가 유용
③ 치료 : Nondisplaced fx. 는 elbow 90도로 flextion 후 long arm posterior splint
(4) Epicondyle fractures
① Uncommon하며 대개는 avulsion fracture.
② 치료 : Elbow 90도로 flextion 후 long arm posterior splint
(5) Condyle fractures
(6) Articular surface fractures
① Trochlea fx.
② Capitellum fx.
(7) Proximal ulna fractures ① Coronoid fx.
② Olecranon fx. ; Ulna n. injury 호발
(8) Radial head fracture
① Radiocapitellar line의 소실, abnormal fat pad sign
② M/C fracture of the elbow
③ Common associate injury
: Capitellum olecranon and coronoid fractures medial collateral ligament injury
: Medial epicondylar avulsion fracture secondary to valgus stress and elbow dislocation.
E. Forearm fractures
•
Radial n.
: 운동 기능 검사는 저항을 주면서 wrist와 finger를 신전시킨다. : 감각은 thumb index web space의 dorsum을 확인 * Median n.
: Ant. interosseous n. function test - "OK' sign을 만든다. : 엄지의 abduction(외전) - median n.의 recurrent br.
: Palm의 radial side의 감각을 확인 * Ulnar n.
: Forearm muscles, intrinsic muscles of the hand : 감각은 little finger and the ulnar half of the ring finger.
E1. Fractures of both radius and ulna
(1) Nondisplaced fx.는 rare
(2) 대부분 수술 (소아 제외)
(3) Compartment syndrome 여부를 감별하는 것이 특히 중요한데 Volkmann's ischemic contracture 방지하기 위함.
E2. Ulna fractures
(1) Isolated ulna fracture (Nightstick fracture)
① Undisplaced fx.는 long arm splint & f/u
② Displaced fx. (10%이상 angulation or fx. site bone 넓이의 50% 이상 전위)는 ORIF
③ Unstable joint - Open reduction & Internal fixation 필요
: >50% 이상 displacement,
: >10% angulation,
: Involve the proximal third of the ulna.
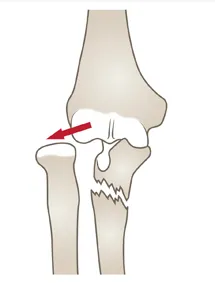
(2) Monteggia fracture-dislocation
•
Fracture of the ulnar shaft with a radial head dislocation
→ ORIF of the ulna & CR of the radial head dislocation
•
소아는 CR of both bones and long-arm cast immobilization
•
Radial head dislocation를 놓치면 chronic pain, limitation of motion이 올 수 있으며 치료로 radial head excision이 필요할 수 있다.
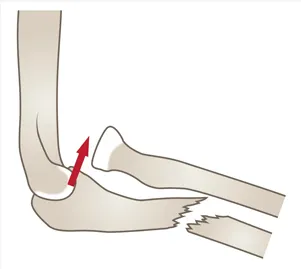
Type I (70%)
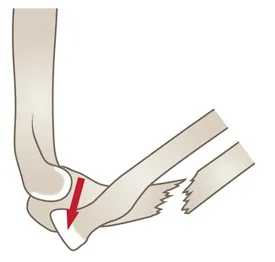
Type II (5%)
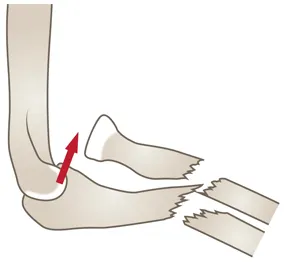
Type IV (rare)
E3. Radius fractures
(1) Proximal 2/3 fx.
① Radial head 포함
② Rotational deformity 예방 위해 internal fixation 요구됨
(2) Distal 1/3 fx. (Galeazzi fx.)
① Fx. of the distal third of the radial shaft, with a distal radioulnar joint dislocation → ORIF ② Ulnar nerve, median nerve의 ant. interosseous branch 손상 : 대부분 spontaneous healing
