

T19. 장에 약물에 대한 좀 더 자세한 기술이 나온다.
A1. 서맥성 부정맥 약물
(1) Atropine
•
0.5~1.0mg (8판에는 0.5mg이라고만 나옴) IV push, 3~5min마다 반복
최대 3mg(0.04 mg/kg)
Sinus bradycardia, junctional rhythm에 효과 있음
2nd degree type II, 3rd degree AV block에는 효과 없음 (특별히 해로움도 없음)
(2) Glucagon : BB, CCB intoxication에 의한 bradycardia에 사용
3~10mg IV over 1~2분, 이후 1~5mg/hr로 유지
A2. AV Node 전도 차단 약물
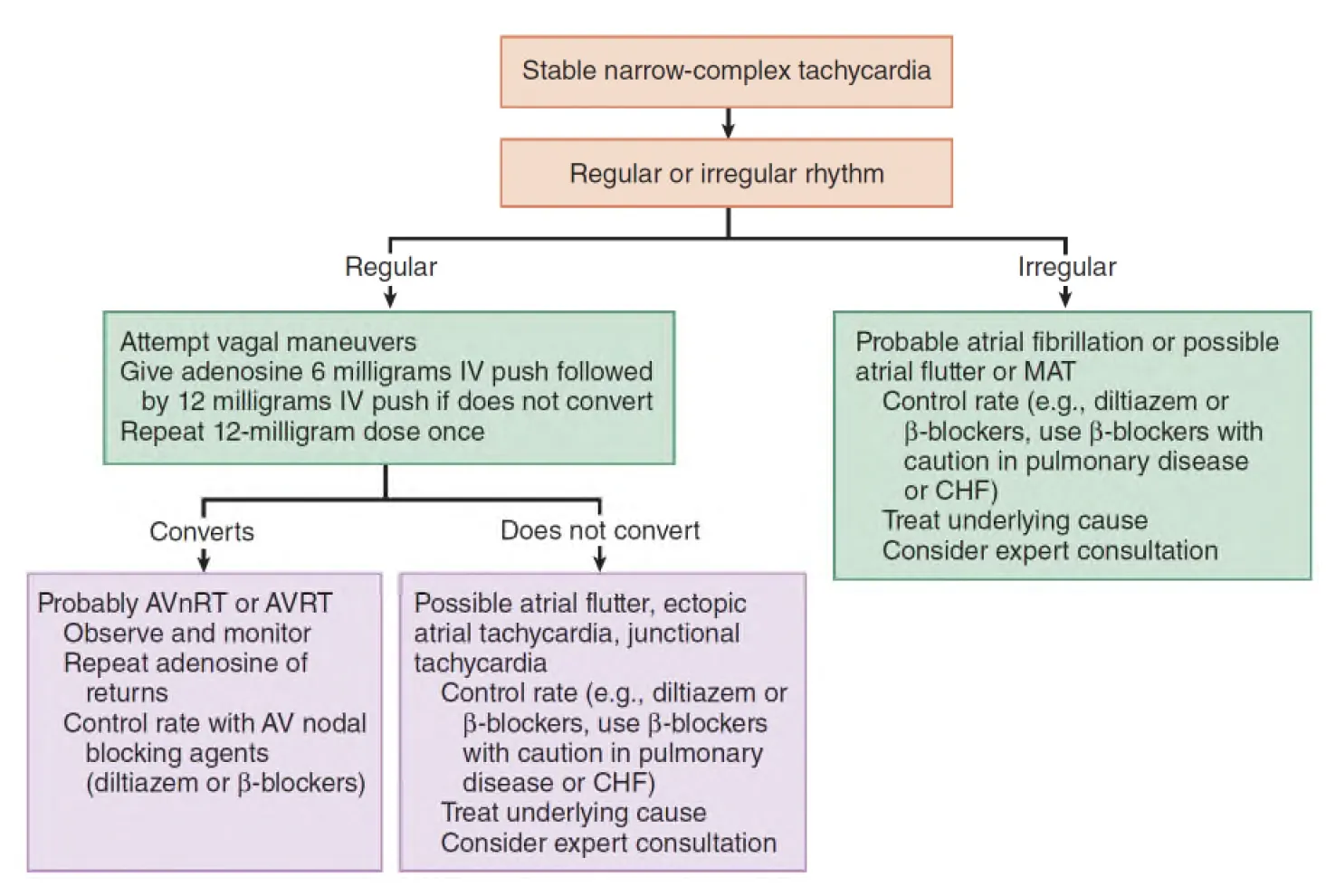
(1) Adenosine
•
6mg rapid IV push; 2분 후에도 지속되면 12mg, 이후에도 지속 시 한번 더
(2) Verapamil
•
5-10mg (8판에서 2.5-5mg) IV bolus over 2~3 min
•
15분 후에도 지속되면 10mg (8판에서 5-10mg)
(3) Diltiazem
•
15~20 mg IV bolus over 2 min, 이후 5~10mg/hr로 유지
initial bolus에 적절한 반응 없을 시 15분 동안 20~30mg bolus 반복 (9판 추가)
verapamil보다 hypotension 유발이 적어 rate control에 주로 사용됨
A3. 빈맥 종결용 약물
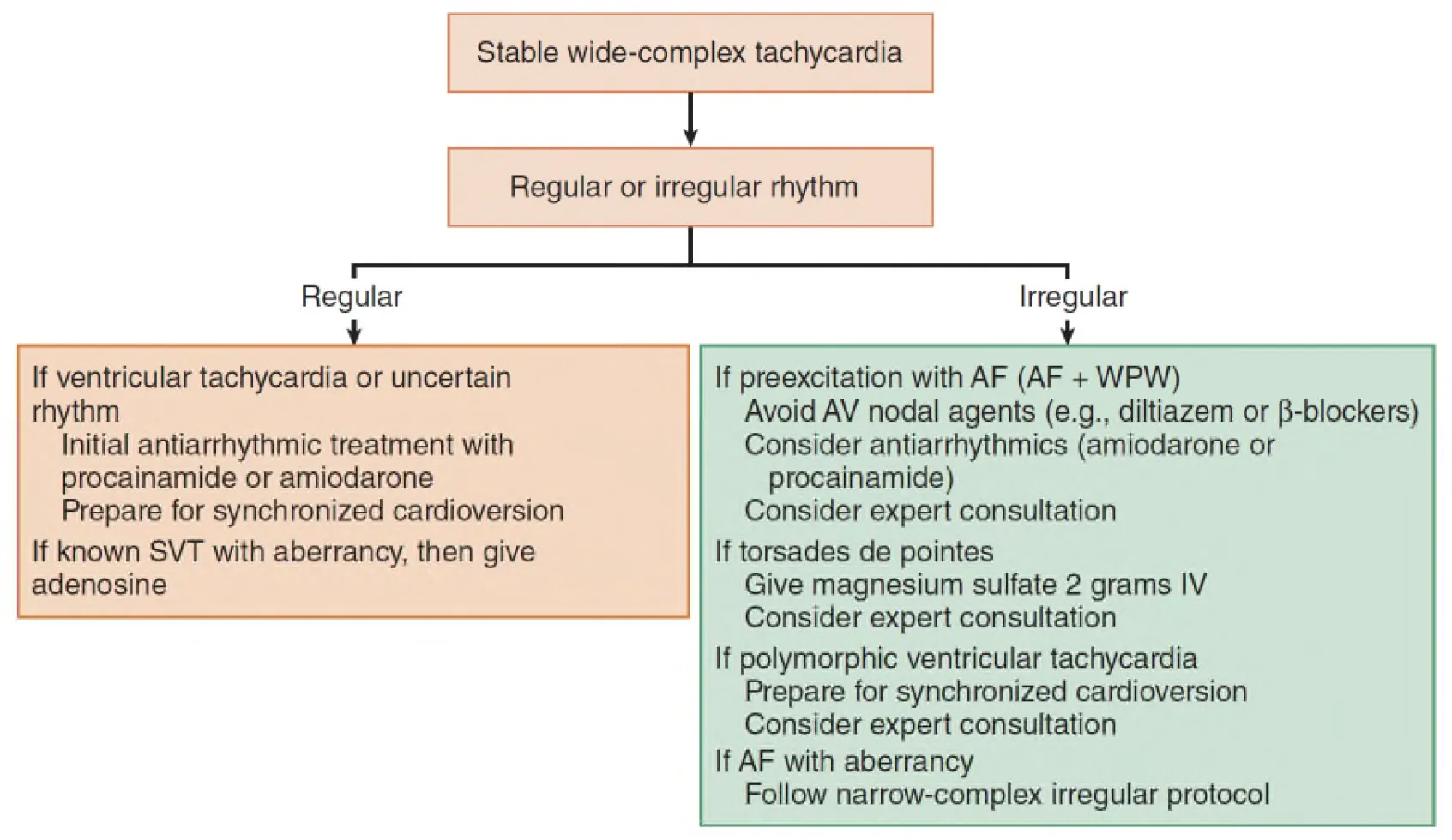
(1) Procainamide
•
Wide-complex tachydysrhythmias and new-onset A. fib
Stable patient의 경우 procainamide가 antiarrhythmic of choice라는 내용이 추가됨.
Initial : 20~50mg/min 혹은 5분마다 100mg 씩 반복 투여
(빈맥이 좋아지거나, 저혈압이 발생하거나, QRS가 기존보다 50% 증가할 때까지
maximum 17mg/kg까지 사용 ), 이후 1-4mg/min 유지 용량
(2) Amiodarone
•
Wide-complex tachydysrhythmias and new-onset A. fib
① Stable patient : 150mg을 5DW 100ml에 섞어서 10분에 걸쳐 투여
이어서 시간 동안 6 1mg/min으로 투여 (9판에서 변경 및 추가)
② VF or Pulseless VT : 300mg IV bolus 이후 추가로 150mg IV bolus
(3) Lidocaine
: 3rd line for VT and VF
Loading dose : 50-100mg을 2~3분 동안, 5분마다 같은 용량으로 반복
(1시간에 최대 300mg까지) 이후 1~4mg/min 유지 용량
(8판-1mg/kg IV over 60초, 5-10분마다 0.5mg/kg로 반복, 최대 1시간에 300mg까지)
(4) Magnesium sulfate : Torsades de pointes with long QT interval
2g IV over 2min, 이후 1~2g/hr로 유지
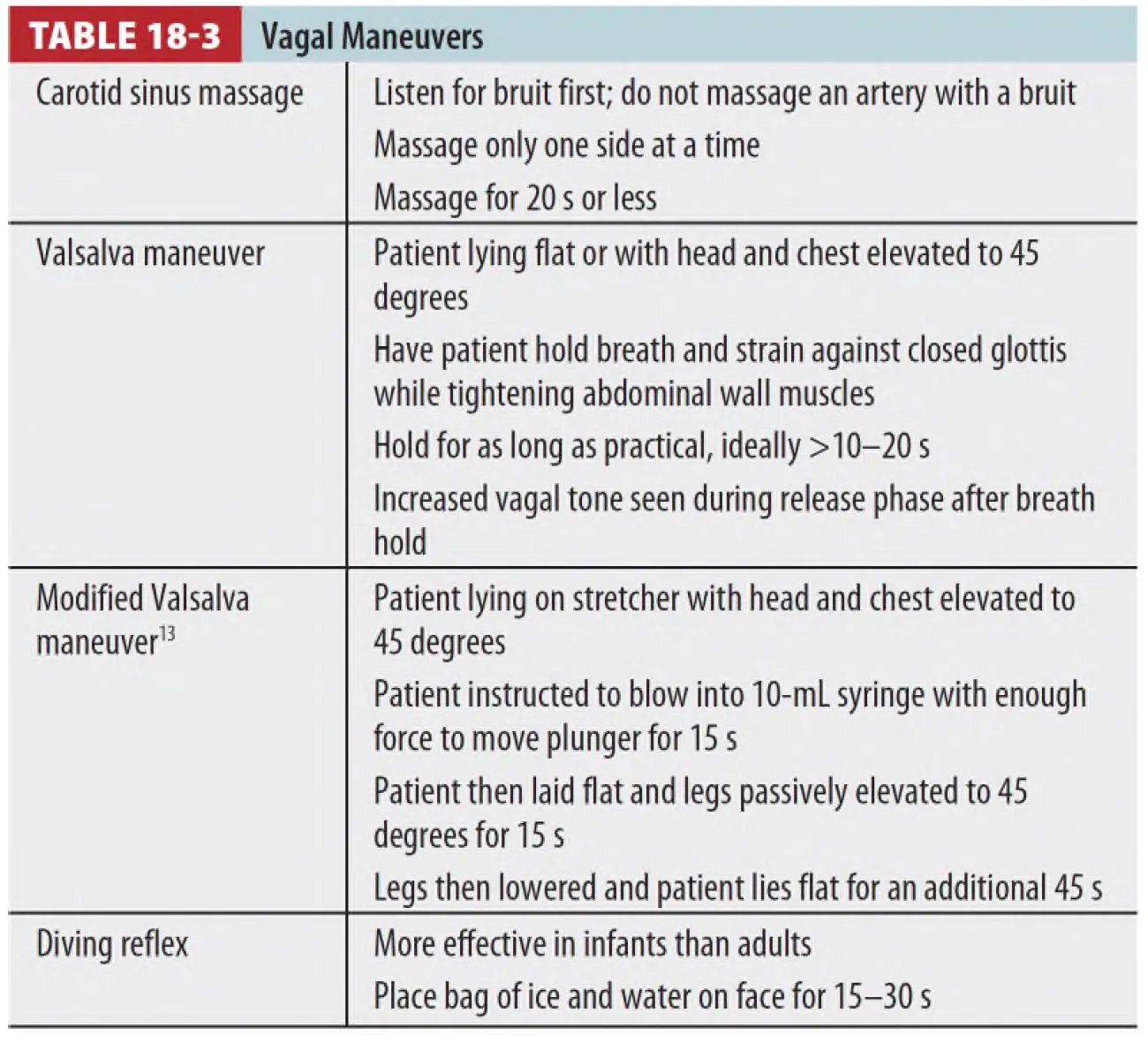
Modified valsalva maneuver가 SVT의 termination에 더 효과적이라고 추가되었음
