

A. Pathophysiology
A1. Visceral pain
•
폐색, 경색, 염증은 unmyelinated fiber를 늘리므로 visceral pain이 발생한다.
(쥐어짜거나, 칼로 베는 듯한, 둔한 양상)
•
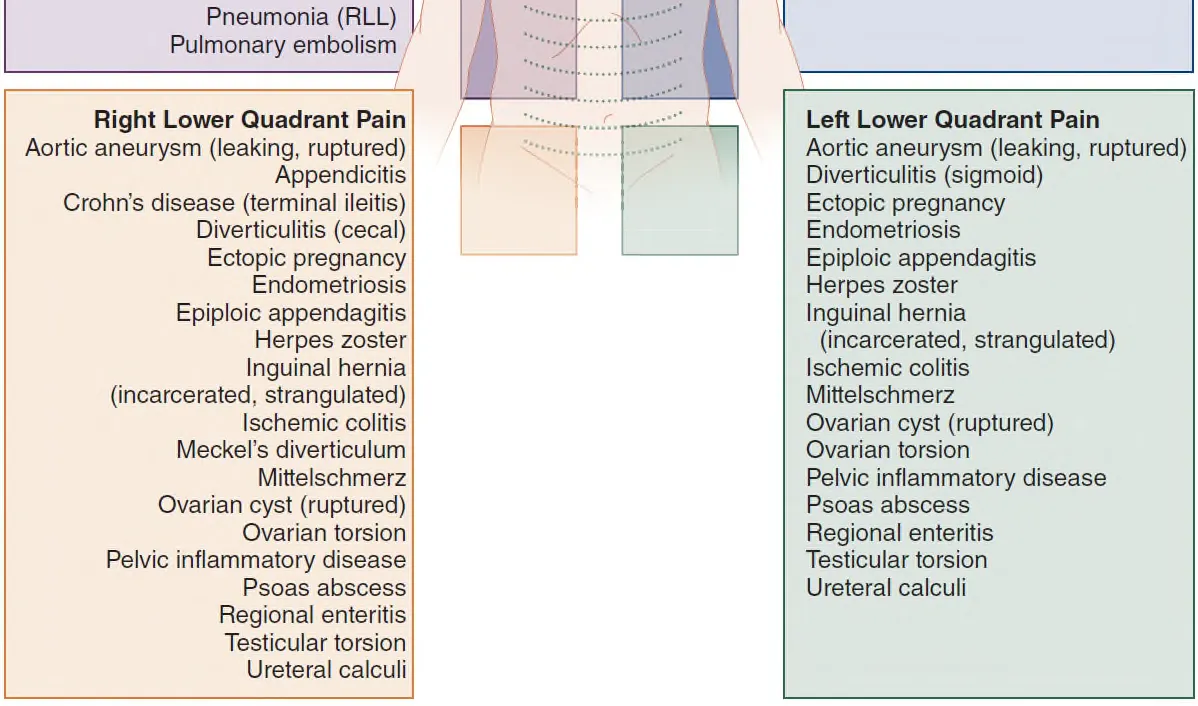
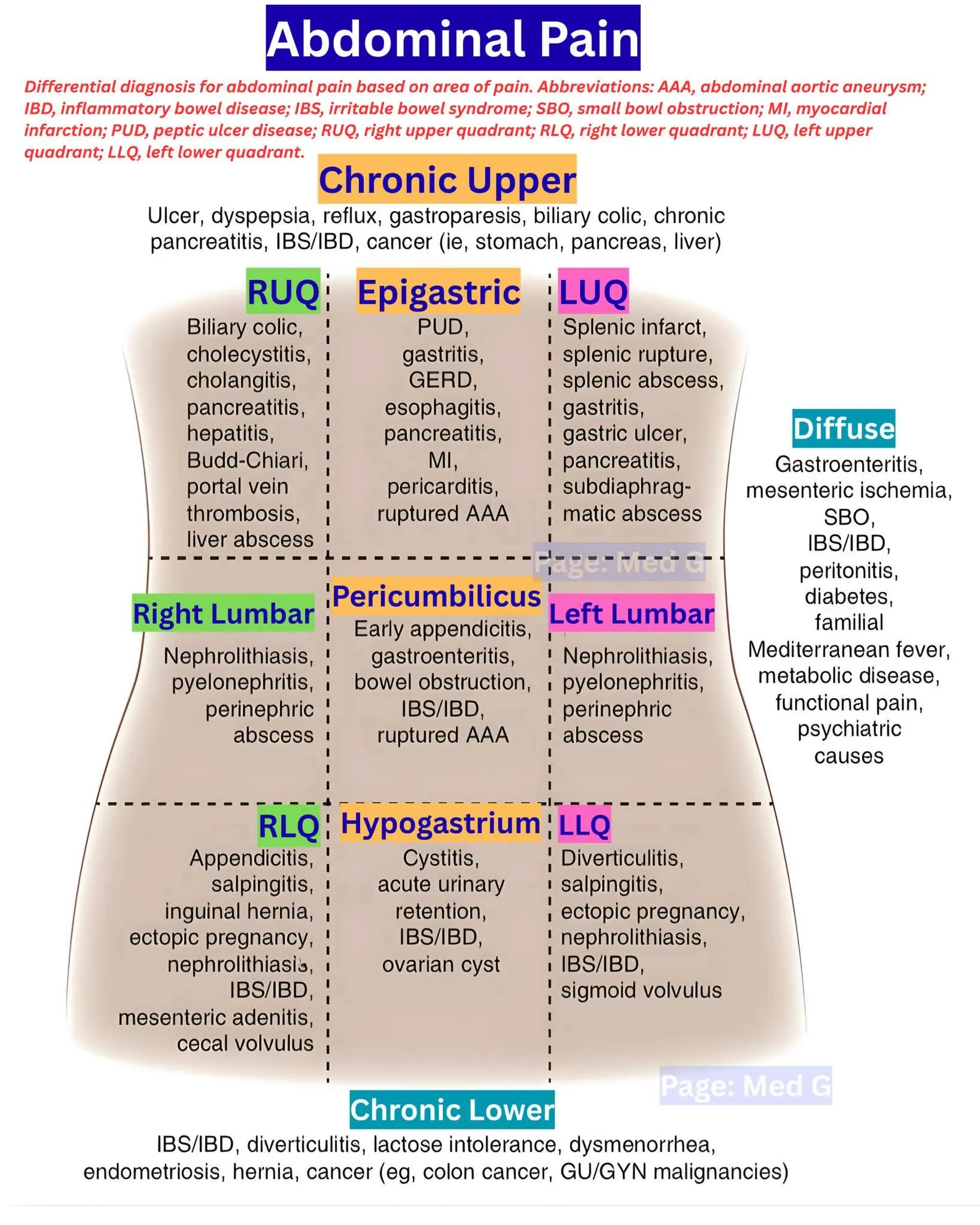
발생계통에 따른 spinal cord level의 sensory cortex를 통해 위치를 예측할 수 있다.
ex) Appendix - t10

A2. Parietal pain
•
Parietal peritoneum을 innervation하는 myelinated fiber의 자극으로 발생한다.
•
Visceral과 다르게, superficial dermatome을 통해 위치를 예측할 수 있다.
A3. Referred pain (방사통)
•
방사통은 발생학에서 연관된 장기끼리 일어날 수 있다.
B. Clinical features
B1. Clinical risk
(1) Patient acuity
•
임상적으로 중환이 의심되면 즉시 안정화 시켜야 한다.
•
고령, 갑자기 발생한 심한 통증, 비정상 활력징후, 탈수, 창백, 식은땀, 토함 등의 증상이 있는 경우
중환일 가능성이 있다.
•
Volume depletion일 경우 혈압은 정상일 수 있고, tachycardia가 중요한 지표가 될 수 있다.
•
Normal blood volume의 30%~40%까지 감소되기 전까지는 수축기 혈압은 유지될 수 있다.
•
체온은 환자의 condition을 판단하는 데 있어서 크게 도움되지 않는다.
(2) Resuscitation
•
Cardiac monitor
•
Oxygen (2 to 4L/min via nasal cannula or mask)
•
Large-bore IV access, and an isotonic fluid bolus
•
AAA를 감별하기 위해 bedside US를 시행하고, 강 내 출혈이 의심되는 경우에는 FAST 확인
(3) Risk factors
•
AIDS 환자에서 CD4 counts가 200/mm3을 넘으면 기회감염의 가능성은 거의 없다.
B2. Physical examination
(1) 통증에 대해 PPQRSTT를 확인한다.
•
Provocative/Palliative factors
•
Quality
•
Radiation
•
associated Symptoms
•
Timing
•
what the patient has Taken for the pain
C. Sx. Tx. and further clinical diagnosis
•
증상의 완화를 먼저 해야 한다.
•
Opioid는 abdominal findings를 모호하게 하지 않을 뿐더러 진단을 늦추거나 혹은 morbidity나
mortality를 증가시키지 않는다.
•
Ondansetron이나 metoclopramide 같은 항구토제의 투여 또한 필요하다.
•
NG tube foley catheter 거치에 대해서도 고려를 해야 한다.
C1. Laboratory testing
•
혈액검사 결과는 착실한 history taking과 P/Ex을 대신하지 않을뿐더러 “routine abdominal labs”
라는 것의 유용성에 대한 검증은 없다.
•
백혈구 수치 단독은 심각한 질환이나 surgical abdomen을 rule out 해주지 않는다.
•
만일 serum creatinine >1.5 혹은 GFR <60인 경우 life-threatening한 경우를 제외하고는
IV contrast는 추천되지 않는다.
(1) Suggested lab studies for goal-directed clinical testing in abdominal pain
Table 71-3
•
Amylase : Pancreatitis (if lipase not available)
•
Lipase : Pancreatitis
•
β-hCG : Pregnancy, ectopic or molar pregnancy
•
Coagulation studies : GI bleeding, end-stage liver disease, coagulopathy
•
Electrolytes : Dehydration, endocrine or metabolic disorder
•
Glucose : Diabetic ketoacidosis, pancreatitis
•
Gonococcal/chlamydia testing : Cervicitis/urethritis, pelvic inflammatory disease
•
Hemoglobin : GI bleeding
•
Lactate : Mesenteric ischemia, sepsis
•
Liver function test : Cholecystitis, cholelithiasis, hepatitis
•
Platelets : GI bleeding
•
Renal function tests : Dehydration, renal insufficiency, acute renal failure
•
Urinalysis : Urinary tract infection, pyelonephritis, nephrolithiasis
•
ECG : myocardial ischemia or infarction
D. Diagnostic imaging
•
이미지 study 역시 history와 physical exam을 대신하지 못한다. 모든 복통이 영상 검사를 필요로 하는 것은 아니다.
D1. 초음파
•
성인에서 담낭, 췌장, 콩팥, 요로, 방광의 용적, 대동맥의 직경을 재는데 도움 된다.
•
소장, 대장 질환에는 도움이 되지 않는다.
D2. APCT
•
만일 serum creatinine >1.5 혹은 GFR <60 인 경우 life-threatening한 경우를 제외하고는 IV
contrast는 추천되지 않는다.
•
AAA rupture or mesenteric ischemia가 의심되는 환자에 있어서는 initial test of choice이다.
E. Treatment
E1. Antibiotics
•
복강 내 패혈증, panperitonitis에서 사용할 수 있다.
•
산부인과적인 원인을 제외한 모든 복강 내 감염은 혐기성균과 G(-) 호기성균을 cover해야 한다.
E2. Dyspepsia 나 Non-specific abdominal pain환자에서 퇴원약
응급실에서 응급원인(외과적/혈역학적/심근허혈 등)을 충분히 배제한 뒤, 기능성/비특이적으로 보이는 acute dyspepsia 또는 non-specific abdominal pain 환자를 퇴원시키는 상황을 전제로 정리한다.canadiem+1
(1) 기본 원칙
•
가능한 한 단기 처방(보통 3–7일) + 증상 호전/악화 시 명확한 FU 플랜.
•
오피오이드는 가급적 피하고, 필요 시에도 최소 용량·단기만 사용.pmc.ncbi.nlm.nih
•
red flag(발열, 체중감소, 지속/악화하는 통증, 토혈/흑색변, 황달, 심한 압통/반발통 등) 발생 시 즉시 재내원 교육.
(2) 1차 선택: 위산 관련 증상(heartburn/epigastric burning 중심)
증상이 명백히 산역류/속쓰림 위주라면 acid suppression을 중심으로 처방한다.
1.
속효성 증상 조절: 제산제 PRN
•
알루미늄/마그네슘 제산제 현탁액 또는 chewable tab PRN (식후·취침 전, 상한 용량 내).
•
ED 연구에서 급성 위통·상복부통에 antacid 단독이 GI cocktail이나 IV PPI보다 단기 통증 조절이 빠른 것으로 보고.tamingthesru+2
1.
지속 증상 예방: PPI 또는 H2 blocker
•
PPI (예: omeprazole 20 mg qd, esomeprazole 20 mg qd, pantoprazole 40 mg qd, 2–4주):
◦
기능성/미조사 dyspepsia에서 1차 약제로 권고되는 경우가 많고, H2RA보다 증상 개선률이 약간 우월.gut.bmj+1
•
H2 blocker (예: famotidine 20 mg bid, 1–2주):
◦
onset이 비교적 빠르고 12시간 정도 acid suppression, 단기 use에 적합.pepcid+1
•
ED setting에서는:
◦
퇴원약으로는 PPI qd 2주 + 필요 시 제산제 PRN 조합이 실용적.
◦
야간 heartburn 위주·증상 경한 경우 famotidine 20 mg hs 또는 bid + 제산제 PRN 도 무난.
(3) 상복부 팽만/조기만복/비특이적 소화불량 위주일 때
•
dysmotility-like functional dyspepsia에서는 PPI 단독이 H2RA + prokinetic보다 우월했다는 연구도 있어 PPI를 여전히 1차로 볼 수 있다.pmc.ncbi.nlm.nih
•
그래도 임상에서는 다음과 같은 조합이 흔함:
◦
PPI qd (또는 famotidine bid)
◦
속쓰림보다는 더부룩함, 조기만복이 prominent할 때 domperidone, itopride 등 prokinetic을 단기(1–2주) 병용 (금기: QT, 파킨슨, 고령 등 개별 고려).
(4) non-specific abdominal pain (원인 미확정, 경증·산통형)
구체적 진단이 안 나오지만 검사상 위험소견 없고, 경증 복통/쥐어짜는 양상인 경우:
•
1차 진통:
◦
PO acetaminophen 500–1000 mg q6h PRN (max 3–4 g/day) ± 짧은 기간 NSAID (위염/신장 위험 고려). 일반 ED 통증 리뷰에서도 NSAID/acetaminophen이 일차 선택으로 제시
◦
경련성 복통이 뚜렷하면:
butylscopolamine, mebeverine 등 진경제를 짧게 PRN 처방 (특히 IBS-like crampy pain).
•
동시에 위장관 원인 가능성이 높으면 위의 PPI/H2RA ± 제산제 중 하나를 추가.
(5) ED에서 피하거나 조심할 약제
•
viscous lidocaine + antacid + antispasmodic “GI cocktail”
◦
제산제 단독보다 우월한 이득이 없고, aspiration·마비성 장폐색 등 잠재 위험으로 인해 routine 사용 비권장.canadiem+1
•
장기 PPI 유지
◦
단기 퇴원 처방(2–4주 후 재평가) 없이 습관적으로 계속 연장되는 경우가 많아, 퇴원 시 이미 종료 시점·추적 계획을 명시하는 것이 좋다.scielo.isciii
•
오피오이드
◦
비특이 복통에서 오피오이드는 진단을 가리고 ileus·변비·구역을 악화시키므로, 구조적 질환이 명확하거나 중등도–중증 통증에서 다른 옵션 실패 시에만 제한적으로.pmc.ncbi.nlm.nih
(6) 실전용 예시 레지멘 (성인, 구조적 질환 배제된 경우)
•
acute dyspepsia (heartburn/epigastric pain 우세)
◦
PPI: pantoprazole 40 mg PO qd × 14일
◦
제산제 현탁액 10–20 mL PO q6h PRN
◦
필요 시 acetaminophen 500–1000 mg PO q6h PRN 복통
•
위팽만/더부룩함·조기만복 우세, 검사상 이상 없음
◦
PPI: esomeprazole 20 mg PO qd × 14일
◦
± prokinetic (예: itopride 50 mg PO tid AC × 7–14일, 개별 금기 고려)
•
non-specific mild abdominal pain, IBS-like cramp
◦
acetaminophen 500–1000 mg PO q6h PRN
◦
butylscopolamine 10–20 mg PO tid PRN (1주 이내)
◦
± famotidine 20 mg PO bid × 7일 (상복부 불편감 동반 시)
이 정도 틀 안에서 환자 연령, 기저질환(신장/간질환, 출혈위험, QT, 파킨슨 등), 현재 복용약을 고려해 조정하면 응급실 퇴원약으로 무난하게 사용할 수 있다.
F. Disposition and follow-up
•
CT 검사 상에서 특이 소견이 보이지 않았다고 하더라도 퇴원 시 진단이 명확하지 않은 경우 12시간 이내에 다시 재내원하도록 교육해야 한다 (Tq 외래에서 받아줘야 말이지).
G. Special populations
G1. Women
•
자궁절제술을 하지 않은 가임기의 급성 복통 환자에서는 정량적 혹은 정성적 소변이나 혈액의 임신 검사결과를 확인해야 한다.
•
특히 혈역학적으로 불안정한 가임기 여성에서는 ectopic pregnancy를 반드시 의심해야 한다.
G2. Elderly patients
•
비록 나쁜 예후(84세 이상, bandemia, free air)와 관련된 확실한 변수들이나, 수술적 처치가 필요한 다른 경우 (저혈압, 비정상적 장음, 심하게 늘어나 있는 bowel loop, 극단적인 leukocytosis)가 없더 더라도 심각한 질환을 배제할 수는 없다.
•
노인 복통환자에서 진단이 불확실하거나 f/u이 잘 되지 않을 것 같은 경우에는 imaging/admission/observation 할 것을 강력히 추천한다 (GE나 NE에서 이런 개념이 없음)
1.
Bariatric surgery patients
2.
Epiploic appendagitis
H. The postop. patient with acute abdominal pain
1.
Ileus and early postoperative bowel obstruction
2.
Acute urinary retention
Table 71-4
(Imaging of) Common diagnoses for acute abdominal pain in adults
1.
Appendicitis - CT preferred in adults and nonpregnant women
2.
Biliary colic - US : 86-96% sensitivity, 78-98% specificity
3.
Bladder outlet obstruction - bedside US
4.
Bowel obstruction - plain films : 77% sensitivity, CT 93% sensitivity
5.
Cholecystitis - US : 91% sensitivity
hepatobiliary iminodiacetic acid scan : 97% sensitivity, 90% specificity
6.
Diverticulitis - CT : sensitivity 93-100%, specificity 100%
7.
Epiploic appendagitis : CT
8.
Mesenteric arterial occlusion - selective CT angiography : 96% sensitivity
9.
Mesenteric venous thrombosis - contrast-enhanced CT
10.
Mesenteric ischemia(nonocclusive) - angiography
11.
Pancreatitis - US may show edema, CT : 78% sensitivity, 86% specificity
12.
Perforated viscus - upright chest x-ray : 80% sensitivity for free air
13.
Ovarian torsion - pelvic US with doppler flow
14.
Renal/ureteral colic - CT
15.
Ruptured ectopic pregnancy - transvaginal US
16.
Ruptured/leaking abdominal aortic aneurysm - bedside US 100% sensitivity
