Changes in leads
Inferior wall infarctions
Anterior wall infarctions
A. Changes in leads
ST segment의 upward displacement는 “myocardial wall injury”를 의미함
Significant Q wave는 “index of necrosis”;
abnormal Q wave는 initial electromotive force의 왜곡을 뜻하며, 이는 곧 reciprocal lead의 initial R wave amplitude증가로 이어짐
T-wave inversion은 “ischemia”를 뜻함; acute infarction 시 T wave 는 inverted되고, 다른 wave에서는 taller
A1. Indicative changes
•
In lead whose positive electrode the wall that is infarcted
•
ST elevation
•
Development of significant Q waves
•
Symmetrical T-wave inversion
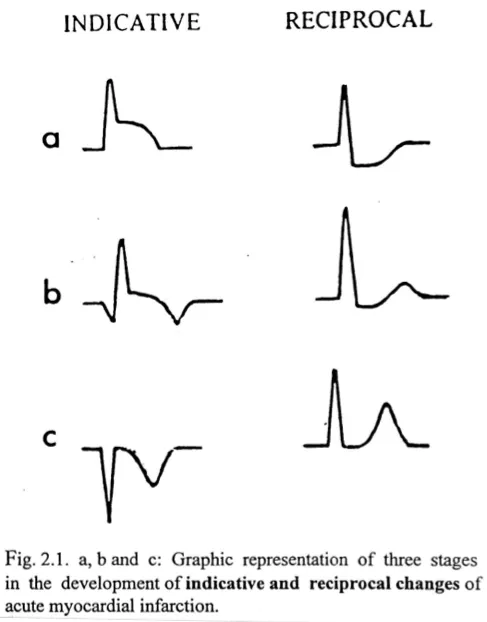
a. ST elevation, ST depression
b. T-wave inversion, increased R wave
c. pathologic Q wave, Tall T
A2. Reciprocal change
ST depression
increase in height of R wave
T waves become symmetrically taller
B. Inferior wall infarctions
B1. Features
•
Straightening of the ST segment with loss of the normal concavity
•
T wave; taller & wider
•
“Saddle-shaped appearance”
•
Reciprocal change; upsloping, horizontal or downsloping ST
•
Early stage; indicative change << reciprocal change
•
Saddle shape appearance 이후 T wave inversion이 진행됩니다.
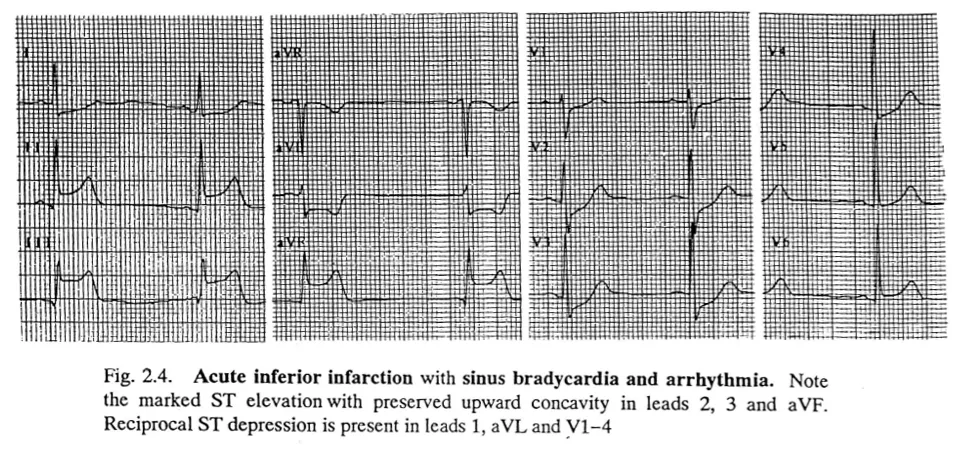
ST-T segment change, Saddle shape appearance, reciprocal change in lead 1, aVL, V1-4
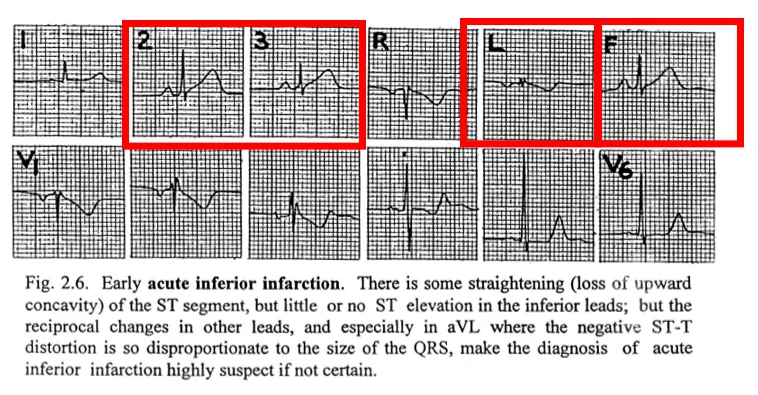
또한 early stage에서는 inferior lead에서의 ST change 저명하지 않은 상태에서 다른 lead, 특히 aVL에서의 qrs와 ST-T 비율의 왜곡을 주목해야합니다.
early acute infarction 시사함
B2. Inferolateral & inferoposterior infarctions
•
V4-6, inferior lead, indicative change -> inferolateral
•
V1-2 Initial R wave height, width increase -> inferoposterior
B3. Complicated inferior infarction
•
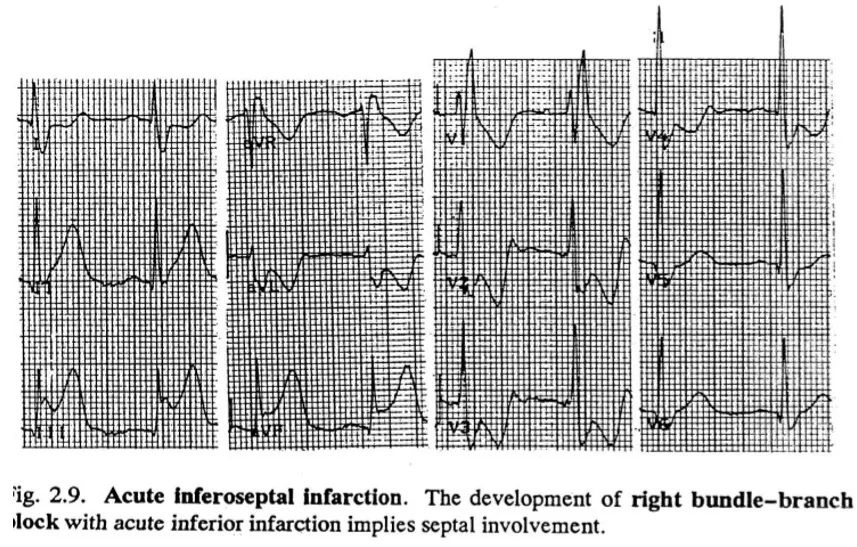
RBBB & inferior infarction -> inferoseptal infarction
•
“Global” infarction
•
Lt. anterior hemiblock
•
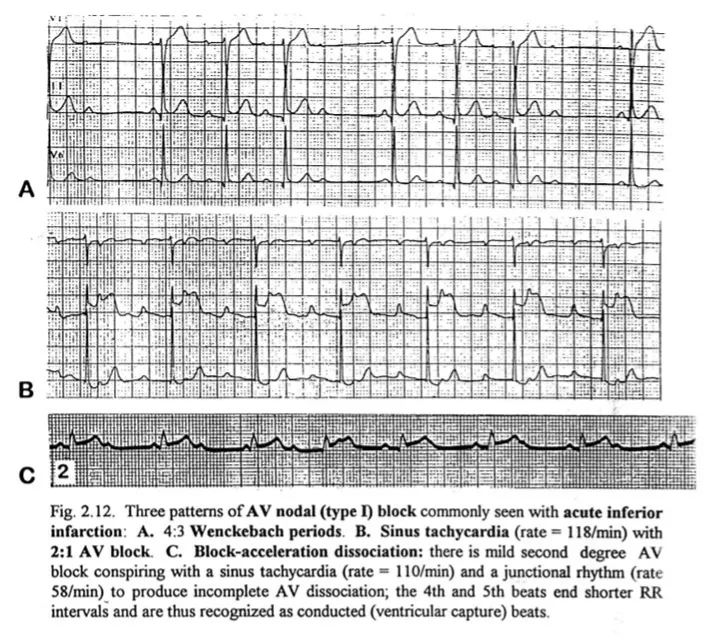
AV nodal block
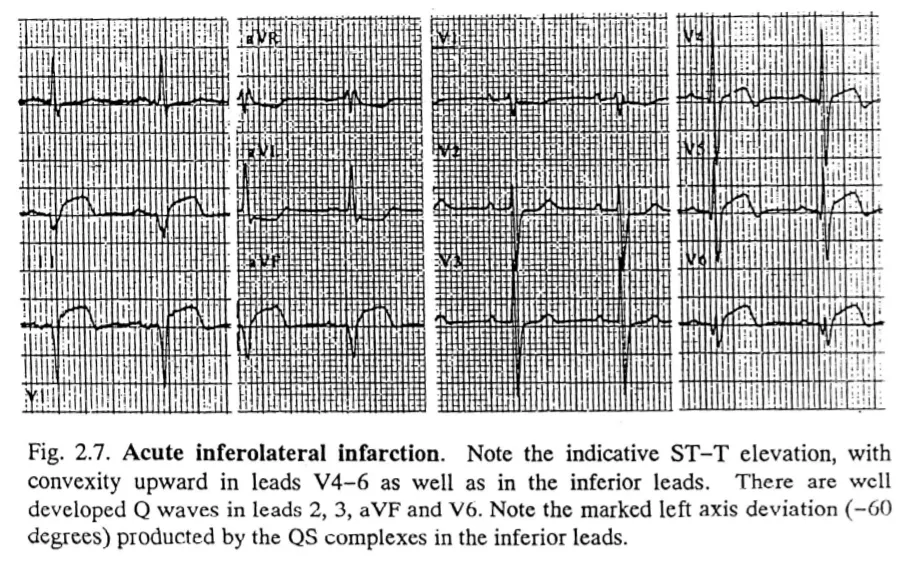
Precordial 4-6포함한 inferior lead의 indicative change 있을 때 inferolateral,
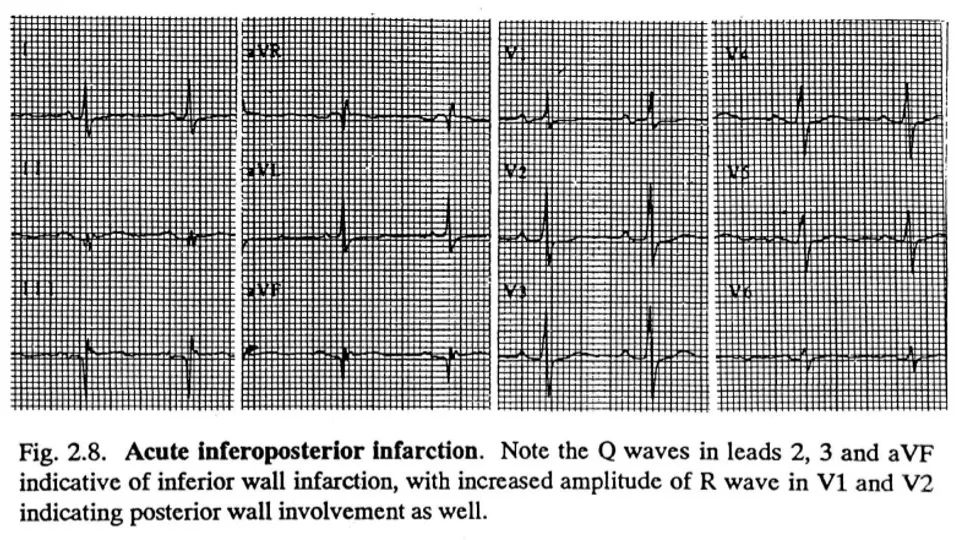
Precordial lead 1-2의 initial R wave height와 width 증가 시 inferoposterior wall infarction 진단합니다.
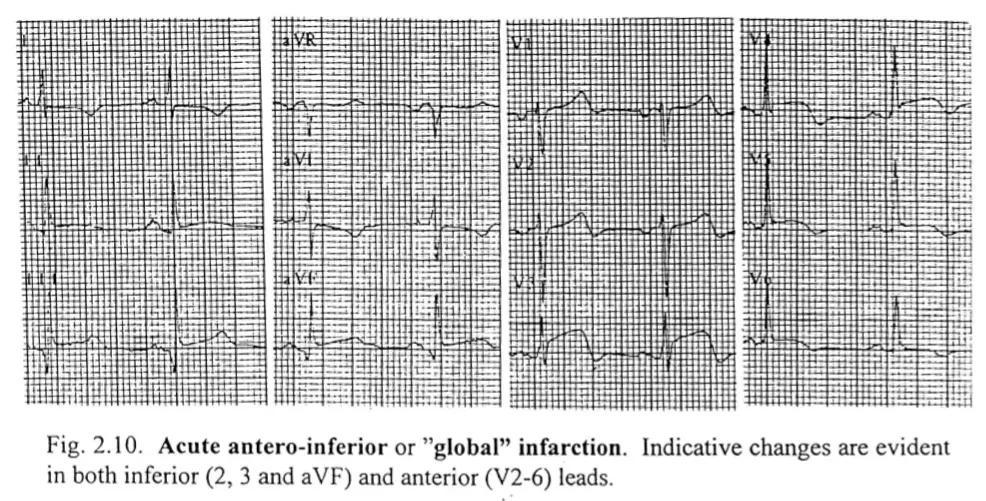
“Global” infarction; p-LAD occlusion (Anterior wall, Apex, Part of the inferior wall)
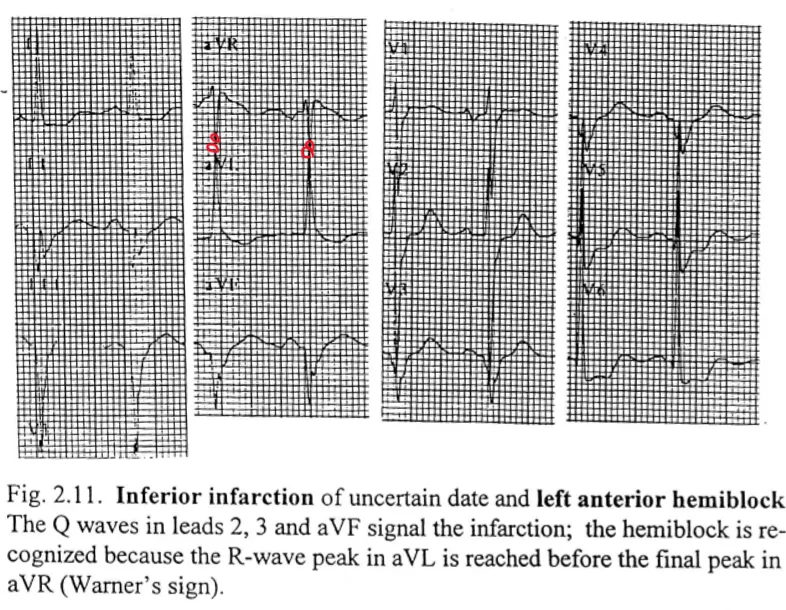
Lt. anterior hemiblock 드물게 발생함. lead 2, 3, AVF deep Q wave, R wave peak in aVL reached before final peak in aVR (Warner’s sign)
C. Anterior wall infarction
•
Anteroseptal & anterolateral infarction
•
V1-4 lead indicative change; anteroseptal
•
V4~ lead indicative change; anterolateral, extensive anterior
•
T wave wide and tall “tombstone T wave”
•
LBBB; infarction Q wave VS LBBB
LBBB 동반 시 infarction은 pathologic Q wave를 만들어내려하고, LBBB는 그와 반대 작용을 합니다. 이에 LBBB 동반된 anterior wall infarctino의 경우 case 중 4/5가량 LBBB의 작용이 우세합니다.
이에 필히 ST curvature, upward concavity를 확인하는 것이 필요합니다.
ST분절 상승 심근경색(STEMI)은 ① 내원 12시간 이내 심근허혈을 시사하는 증상이 있고(증상이 사라졌더라도), ② 12유도 심전도상 J-point 기준으로 연속된 2개 이상의 유도에서 ST분절의 상승이 있는 경우 즉각적인 재관류처치를 권고한다.
심전도상 심근경색의 기준은 V2~3 유도에서는 J-point에서 ST분절 상승이 남성은 0.2 mV, 여성은 0.15 mV 이며, 이외의 유도에서 0.1 mV로 정의된다. 그러나 이전의 심근경색 과거력 및 좌각차단 등 전도 이상이 있는 경우 다른 기준이 적용된다.
•
급성심근허혈을 시사하는 심전도 소견(좌각차단이 없는 경우)
ST분절 상승 : 2개의 연속된 유도에서 J-point에서 새로운 ST분절의 상승이 있는 경우
- V2~3 유도
40세 미만 남성 : 0.25 mV 이상
ST분절 저하 및 T파의 변화
- 2개의 연속된 유도에서 현저한 R파 혹은 R/S > 1을 동반한 T파의 역변화 ≥ 0.1 mv
* 급성관동맥질환/협심증을 시사하는 심전도 소견
ST segment 상승/하강 | Upward convex elevation ± reciprocal change
More 2 consecutive leads
Symmetrical deep T-inversion
Dynamic ST-T change |
Q wave duration > 0.04 sec (1 mm)
Q wave amplitude > 1/4 of QRS
Any Q wave in V1~2 precordial leads | |
RBBB
LBBB | |
* Most important finding : New-onset |
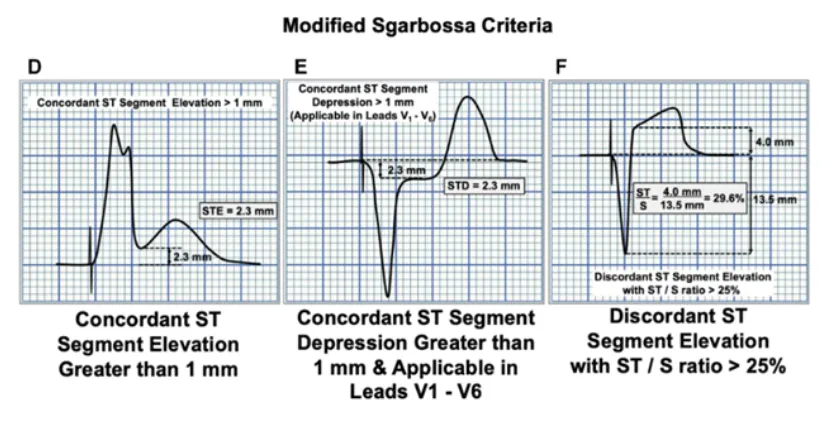
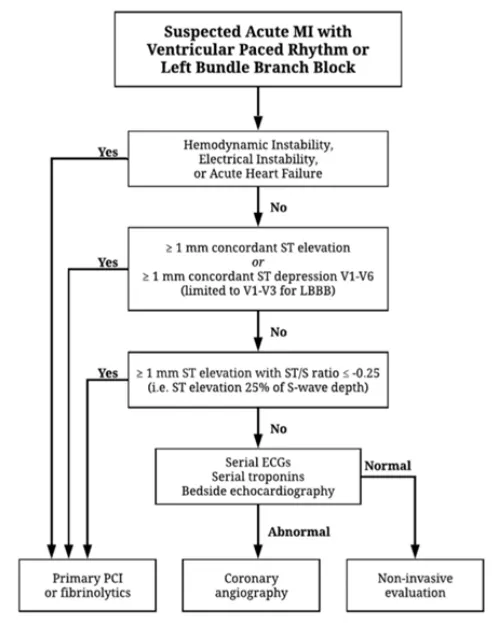
※ Modified Sgarbossa Criteria