
I. Introduction
1. Hemophilia : Clotting cascade에 필요한 factor의 결핍으로 나타나는 출혈성 질환
(1) Factor VIII 결핍 : hemophilia A
(2) Factor IX 결핍 : hemophilia B
2. vWD : vWF의 유전적 결핍 → PLT, 응고인자 둘 다 문제
3. 작은 외상이나 마이너 수술에서 심한 출혈이나 자발적 출혈을 보일 시 의심 (특히 관절, 근육)
4. Spontaneous deep bruises, hemarthrosis, retroperitoneal bleeding, intracranial bleeding
있는 환자 → Coagulation factor deficiency 의심
II. Hemophilia
1. Epidemiology
(1) Hemophilia A >> hemophilia B : 합치면 유전적 coagulation factor deficiency의 99%.
(2) X-linked disorder : 남성이 대부분, 여자는 대게 무증상 carrier나 증상이 있는 경우도 있다
(3) Spontaneous gene mutation에 의한 경우가 있으므로 가족력이 없을 수도 있다.
2. Pathophysiology
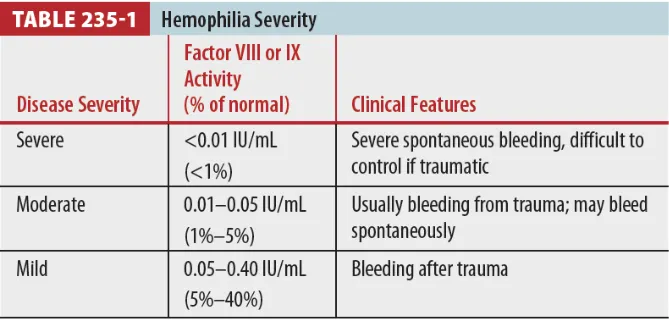
(1) Factor activity level에 따라서 다양한 임상 양상을 보인다.
(2) 정상 수치의 30~40% (0.3~0.4 IU/ml) 까지는 출혈 경향이 뚜렷하지 않을 수 있다.
3. Clinical features
(1) Easy bruising, joint & muscle에 반복적인 bleeding이 특징적임.
(2) 외상, 수술 후 지혈이 어려움, abdomen, retroperitoneum, CNS 출혈도 가능함.
(3) 모계 가족력 반드시 확인.
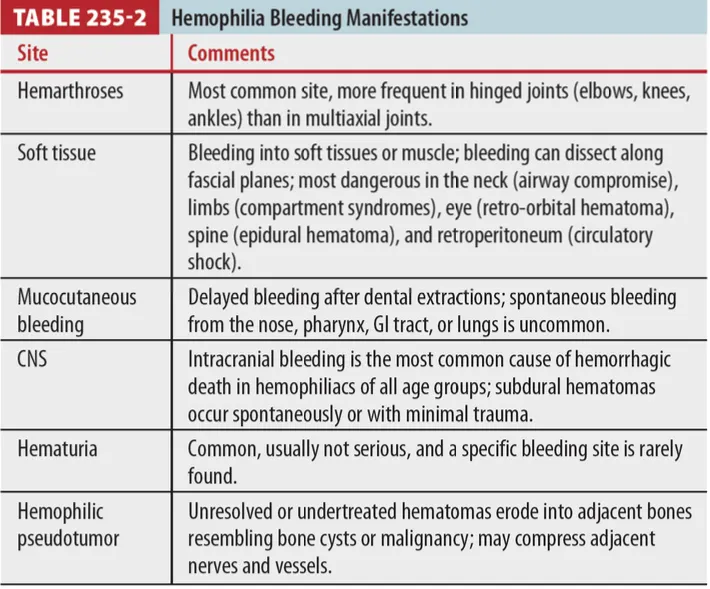
(4) Spontaneous 또는 trauma로 설명할 수 없는 (심한) joint, muscle 또는 CNS bleeding
(Table 235-2)
4. Diagnosis
(1) PT (extrinsic coagulation cascade 반영) : Normal
(2) aPTT (intrinsic coagulation cascade 반영)
1 Abnormal
2 Mild hemophilia에선 normal 일수 있다. (factor activity가 normal의 30~40% 이상)
(3) BT : Normal, not helpful
(4) 확진 : Factor VIII, IX level의 정량 측정시 <0.50 IU/mL (<50%)
(5) 여성 carrier 및 산전검사
: 유전자 검사 확진, Chorionic villus sampling (9~14주), Amniocentesis (15~17주)
5. Treatment
(1) General principles (Table 235-3)
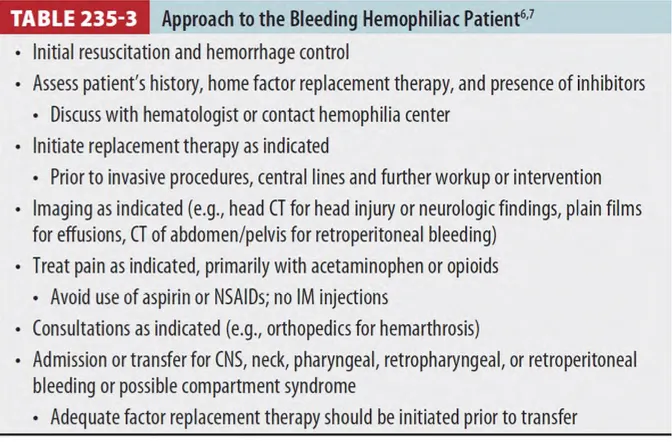
1 Major or life-threatening bleeding
: Factor replacement 우선 시행해야 함
: Intracranial, intrathoracic, intra-abdominal, retroperitoneal, ocular, airway bleeding 등에
대한 처치
: 검사보다 먼저 혹은 동시에 replacement 진행해야 함
2 Neck, tongue, retropharynx, pharynx에 bleeding : Airway 유지 필요
3 Intracranial hemorrhage가 의심되는 상황 (acute severe headache, blunt head injury 후)
: Brain CT scanning 전에 factor replacement therapy 먼저
4 Iliopsoas muscle bleeding은 retroperitoneal bleeding 중 흔한 형태
: Hip pain 호소
: 다리 뻗기 힘들어 하고 flexed, external rotation 상태로 유지하려 함
: Femoral nerve 압박되고 손상, 실혈로 인한 anemia 및 circulatory shock 유발 가능
5 Muscle bleeding
: Compartment syndrome 가능
: Factor replacement 후에 compartment pressure 측정
6 Hemarthrosis
: 가장 흔한 증상 중 하나
: Hemophilic arthropathy의 long-term sequelae를 예방하고 줄이는 것이 목표
7 초기 출혈은 subtle하고 benign하여 initial 검진에서 출혈이 명확하지 않을 수 있으나 추후 출혈이
있을 수 있음을 환자에게 주지시켜야 함
8 Central line, ABGA, lumbar puncture, IM injection
: Factor replacement 우선 시행
: Invasive procedure 전에는 factor replacement 먼저 시행할 것!
9 통증 조절 시, aspirin이나 NSAIDs 포함된 제제는 금기
10 병원 간 전원 갈 때도 factor replacement 후에 transfer
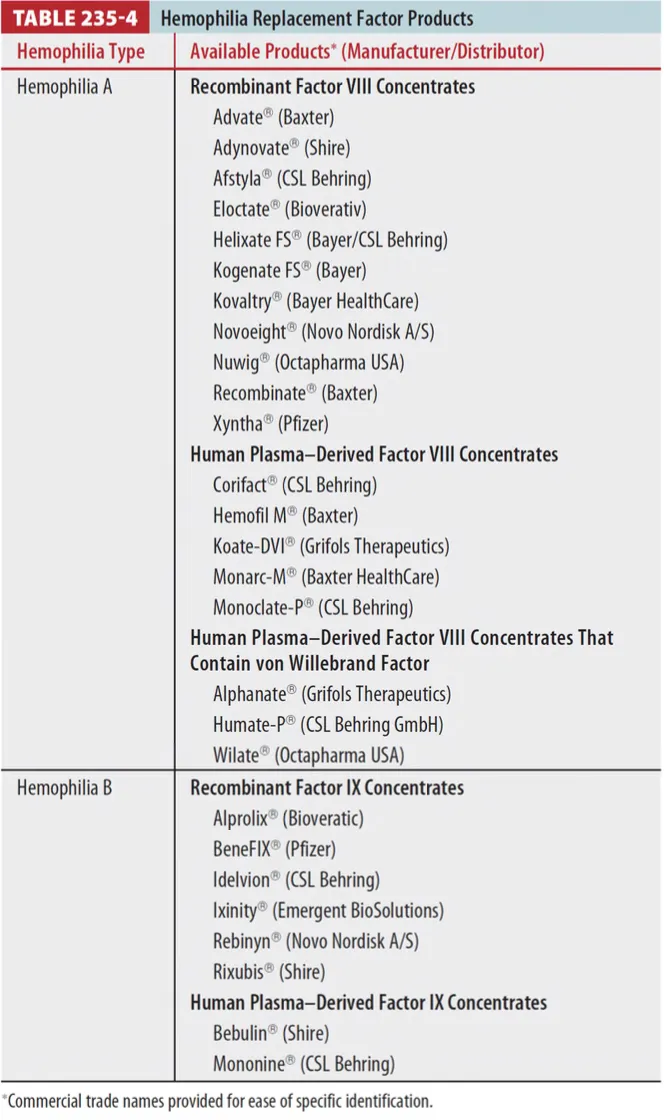
(2) Factor replacement therapy
•
Factor 재료는 2가지 종류가 있다. (Table 235-4) 가능하면 환자가 사용하던 종류 factor를 써야 함.
1 Purification from human plasma
2 Recombinant technology from hamster or human embryonic kidney cell lines
: 사용 용량은 여러 가지를 고려하여 결정한다. (Table 235-5)
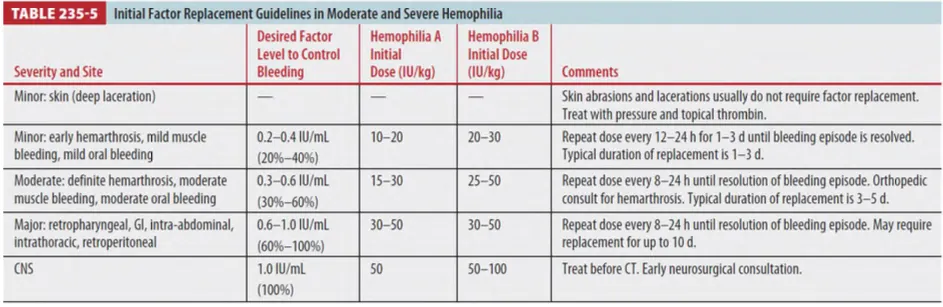
: Factor VIII - 반감기 8~12시간 / kg당 1unit 투여 → Plasma level이 2% 상승
: Factor IX - 반감기 16~24시간 / kg당 1unit 투여 → plasma level이 1% 상승
: Cryotherapy - Hemarthrosis에 대한 benefit이 증명되지 않음
6. Special considerations
(1) Oral & mocosal bleeding
1 입에서 bleeding은 성인보다는 소아에서 더 흔한 증상이다.
2 Bleeding area 확인
→ Inadequate clot 제거 → Topical bovine thrombin spray or gelatin sponge apply
3 Severe bleeding 시 factor replacement + Antifibrinolytic agents
(ex. Aminocaproic acid & Tranexamic acid)
(2) Mild hemophilia A (factor level이 normal의 5% 이상)
1 Mild bleeding 시 항상 factor replacement가 필요하지는 않음
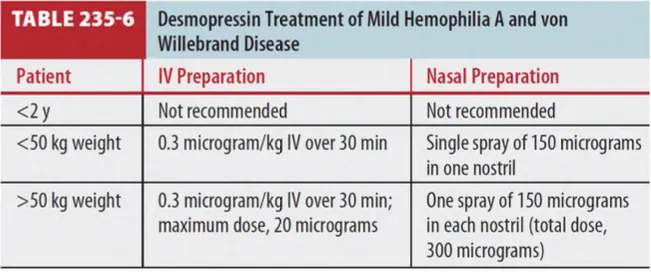
2 Desmopressin 투여 (Table 235-6)
: Endothelial cell에서 vWF 분비 자극 → vWF 증가 → plasma의 factor VIII 운반 증가
: 반복투여 가능하나, 저장돼 있던 factor VIII가 소진되면 desmopressin 효과 감소
: Antidiuretic agent이기 때문에 fluid restriction 필요, intranasal form은 가정에서 많이 쓰인다.
(3) Hematuria
1 흔한 증상이나 대체로 severe 하지 않음
2 Rest & hydration이 중요함
3 Gross hematuria 시 Factor replacement
4 Nephrolithiasis 의 risk factor
(4) Factor inhibitors
1 Replacement factor에 대한 antibody : severe hemophilia 환자에서 흔하게 관찰됨
2 Factor replacement 효과 저하 및 factor replacement 시에 anaphylaxis도 유발 가능
3 Inhibitor가 있는 hemophilic 환자 치료 시
: Inhibitor titer가 적고 (<5 Bethesda inhibitor assay) 환자가 Ab에 강한 반응을 보이지 않는 경우
→ Factor 용량을 증량해서 존재하는 Ab를 압도하도록 준다.
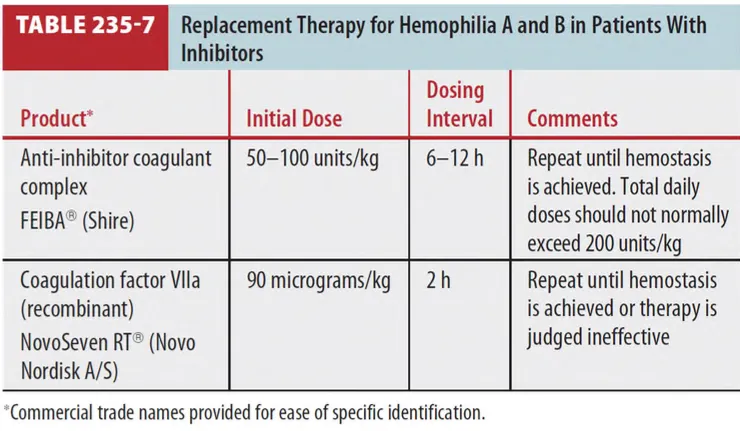
: 다른 방식의 replacement therapy를 시행한다. (Table 235-7)
(5) Acquired hemophilia
1 Factor VIII에 대한 autoantibody가 생성
2 Purpura 나 internal bleeding 주로 발생, hemarthrosis는 드물다.
3 급성 출혈 시 치료는 inhibitor antibody를 피하기 위해 anti-inhibitor coagulant complex나
coagulation factor VIIa (recombinant)를 사용한다. (Table 235-7)
(6) Postpartum acquired hemophilia
1 드물지만 심한 출혈의 가능성이 있다.
2 첫 번째 임신을 하고 출산 2개월 후에 가장 위험, 질출혈이 가장 흔한 증상이다.
3 출혈에 대한 치료는 anti-inhibitor coagulant complex나 coagulation factor VIIa (recombinant)
사용한다. (Table 235-7)
4 Autoantibody 형성은 수개월이 지나면 점점 줄어들어서 결국에는 remission 되고 두 번째 임신에서
재발은 드물다.
7. Disposition & Follow-up
(1) Typical joint, soft tissue, nasal bleeding : 응급실에서 initial treatment 후 퇴원 가능
(2) 입원 적응증
1 Multiple factor replacement
2 Parenteral pain control 필요 시
3 Bleeding (CNS, neck, pharynx, retropharynx, retroperitoneum)
4 Compartment syndrome 가능성 있을 경우
III. von Willebrand’s disease
1. Epidemiology
(1) 가장 흔한 선천적 bleeding disorder (인구의 약 1%)
(2) 대부분 경한 증상, 심한 출혈은 1% 정도
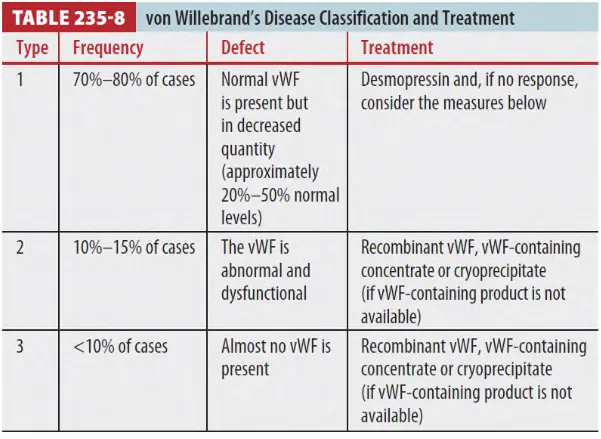
(3) Congenital vWD : 3 major groups (Table 235-8)
(4) Acquired vWD : autoAb to vWF
2. Pathology
(1) vWF : vascular endothelial cell에서 합성, 저장, 분비됨. 지혈 과정에서 2가지 key role
(2) Platelet adhesion의 cofactor
: vWF가 subendothelial matrix 에 노출 → vWF 의 구조적 변화 → Plt glycoprotein Ib에 결합
→ Plt activation & adhesion
(3) factor VIII의 carrier protein
: vWF는 plama 내의 proteolytic degradation으로부터 factor VIII를 보호
3. Clinical features
(1) Skin, mucosal bleeding이 흔함 :
Recurrent epistaxis, gingival bleeding, unusual bruising, GI bleeding, menorrhagia
(2) Hemarthrosis는 드물다.
(3) Mild 한 경우에는 모르고 사는 경우도 많다.
4. Diagnosis
(1) Bleeding time 연장, vWF antigen 감소 혹은 정상, vWF activity 감소
(2) PT 정상, aPTT 약간 연장 (환자의 절반 정도)
(3) Mild hemophilia A와 감별진단이 어려울 수도 있다.
5. Treatment
(1) Nontransfusional therapy
1 Desmopressin
: Type 1 vWD 환자의 일차 치료, endothelium 내 저장소에 있는 vWF 분비를 유도함
(vWF 일시적으로 2-4배 증가)
: Desmopressin은 endothelium에 hemostasis를 촉진하는 역할도 한다
2 반복해서 사용 가능 : 저장돼 있던 vWF가 소진됨에 따라 효과 감소
3 IV 및 intranasal spray도 사용 가능함
4 사용 후에는 24시간 동안 fluid restriction이 필요함. (Hyponatremia 방지)
(2) Transfusional therapy
1 Desmopressin에 반응 없는 type 1 vWD & type 2, 3 vWD 환자
2 vWF를 함유한 plasma derivatives 사용 (Table 235-4)
3 Cryoprecipitate : Factor VIII과 vWF 함유했으나 viral inactivation 과정을 거치지 않았기 때문에
life-threatening emergency에서 factor VIII concentrates 충분하지 않을 때만 써야 함
4 Platelet : vWF products에 반응하지 않는 type 3 vWD 환자
(3) Additional therapy
1 Antiplatelet effect를 가진 약은 금기
(Aspirin, NSAIDs, Antiplatelet agents, Heparin, 일부 antibiotics 등)
2 Significant epistaxis
: Desmopressin이나 수혈, 효과 없으면 intranasal topical therapy 나 cauterization 필요
3 Menorrhagia가 young women에서 흔함 : Oral contraceptives
4 Dental injury 또는 oral cavity 내 계획된 시술
: Antifibrinolytic agent (Aminocaproic acid, tranexamic acid)
6. Disposition & Follow-up
(1) 대부분 vWD 환자의 bleeding episodes는 국소적 처치 및 desmopressin으로 조절됨
(2) 입원 적응증
1 Multiple factor replacement
2 Parenteral pain control 필요 시
3 Bleeding (CNS, neck, pharynx, retropharynx, retroperitoneum)
4 Compartment syndrome 가능성 있을 경우
