B1. Epidemiology
(1) 6~12개월 연령에서 가장 많이 걸림
(2) Risk factor : male, FHx of recurrent AOM, day care attendance, early occur (<1세), atopy
 모유수유는 protective 효과 있음
(3) 40℃ 이상의 고열은 흔치 않으며 고열이 있는 경우 타진단 고려 필요
모유수유는 protective 효과 있음
(3) 40℃ 이상의 고열은 흔치 않으며 고열이 있는 경우 타진단 고려 필요
모유수유는 protective 효과 있음
(3) 40℃ 이상의 고열은 흔치 않으며 고열이 있는 경우 타진단 고려 필요B2. Pathophysiology
(1) 소아의 Eustachian tube가 더 짧고 수평적이다
(2) Bacteria와 virus가 combine 되어 병을 일으키는 경우가 제일 많음
(3) Bacterial pathogen
: S. pneumoniae (49%), nontypeable H. influenzae (29%), M. catarrhalis (28%)
(4) Viral pathogen
: Rhinovirus, enterovirus, RSV, Parainfluenza virus
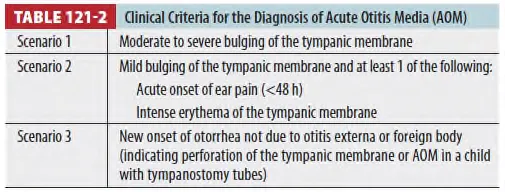
B3. Diagnosis
(1) 고막의 Erythema 단독으로는 AOM 진단으로는 불충분하다.
(중이의 염증이나 울음, 열에 의해서도 생기므로)
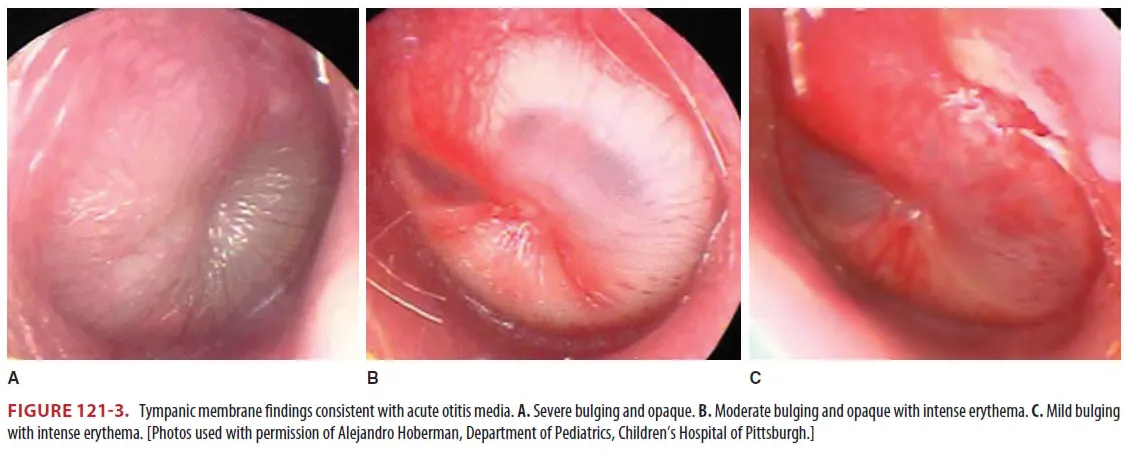
(2) Bulging이 있는 지 확인 (★)
B4. Treatment
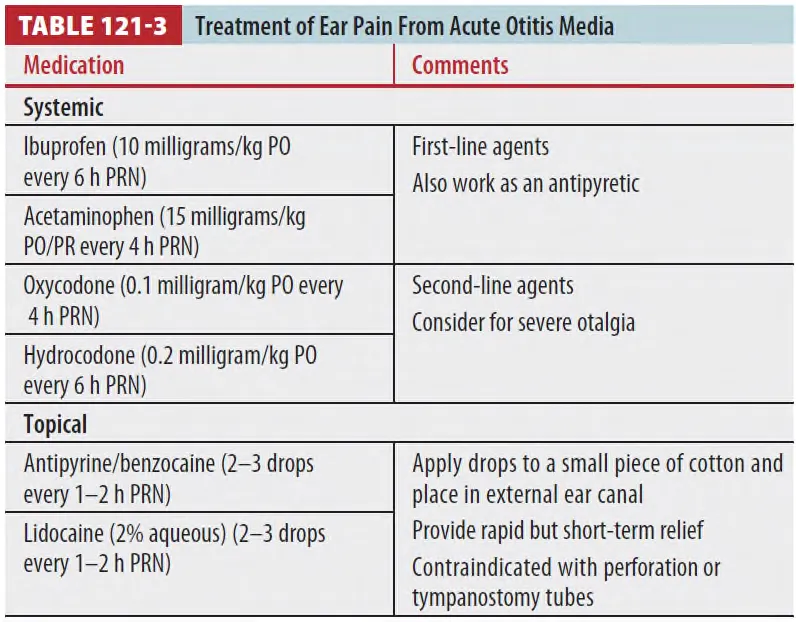
(1) 통증 조절
•
가장 중요함
•
Topical analgesics는 perforation나 tympanostomy 시에는 금기이다.
(2) 항생제 치료 (★)
•
First line
: high-dose amoxicillin, 40~45mg/kg twice a day PO로 5~10일간
: Higher dose를 사용하는 이유는 가장 흔한 원인균인 s. pneumoniae의 minimum inhibitory
concentration 이상의 농도를 유지하기 위함임.
•
Second line : Amoxicillin 치료 실패 시 Amoxicillin/clavulanate or Ceftriaxone
•
Third line : Clindamycin and 3rd general cephalosphorin
•
항생제 사용 후 24~48시간 동안은 발열, 이통이 지속될 수 있으나, 72시간이 넘어가면 재평가,
약물 변경을 고려해야 함.
•
PO 복용이 어려운 경우 IM or IV ceftriaxone 3일간 투여도 가능함
•
Penicillin allergy가 있는 경우 macrolide (azithromycin) 투여 가능
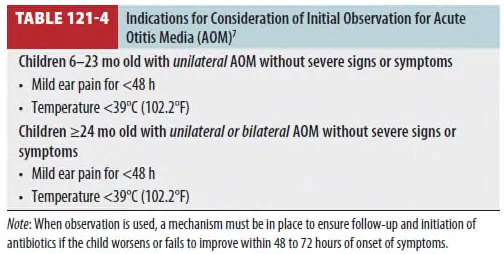
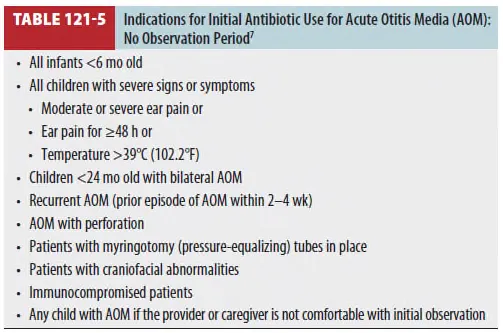
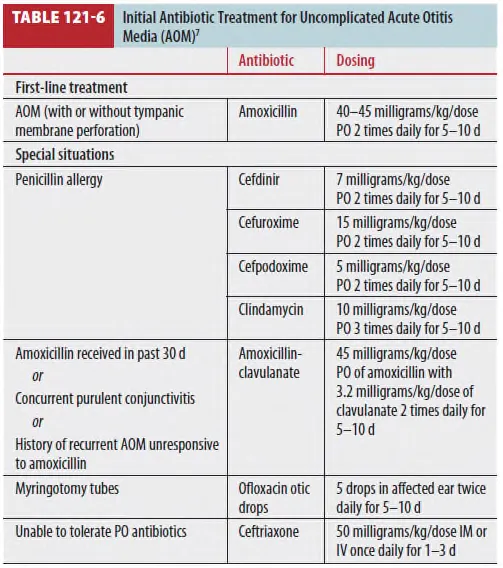
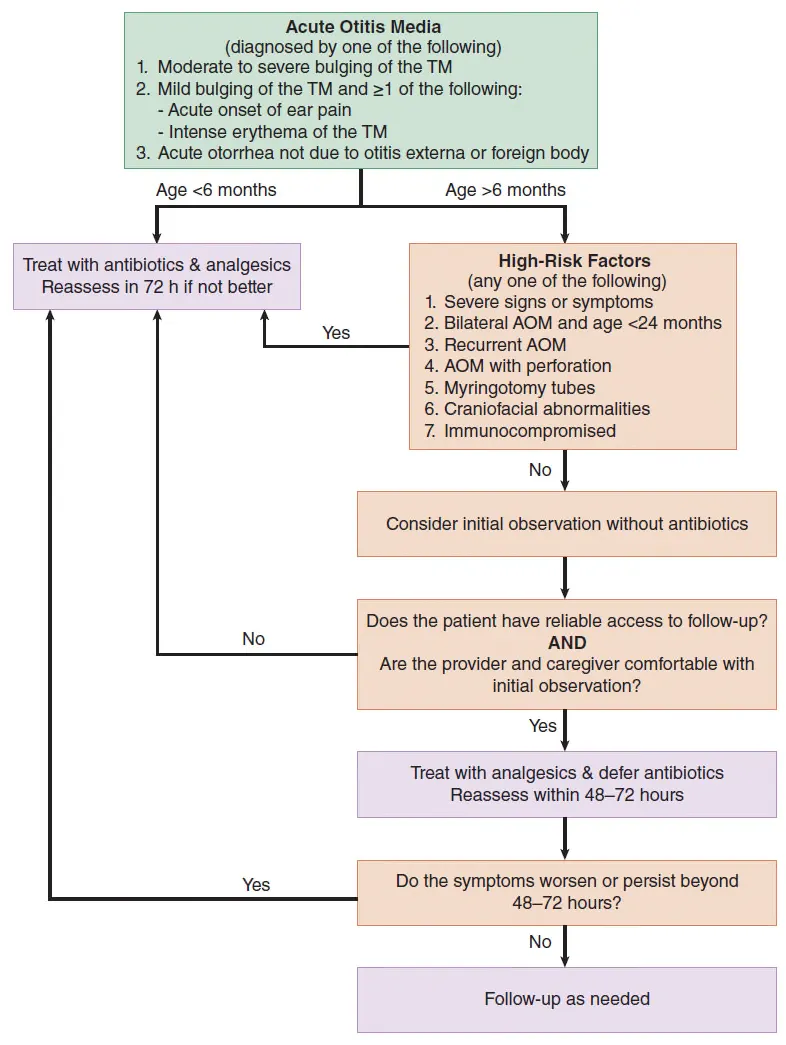
Fig 121-1. Algorithm for management of acute otitis media