A.STEMI criteria
•
V2-V3 제외 인접한 두 lead에서 >0.1 mV (1 mm)
•
V2-V3
◦
40세 이상 남성은 ≥ 0.2 mV (2 mm),
◦
40세 미만 남성은 ≥ 0.25 mV (2.5 mm),
◦
여성은 ≥ 0.15 mV (1.5 mm)
A1. V2-V3 lead에 나이와 성별을 고려하게 된 이유
•
정상인에서 남성이 여성보다 특히 precordial lead 의 ST amplitude가 높다
•
남성에서 특히 나이가 감소함에 따라 ST amplitude가 감소하는 양상 보임
•
STEMI 환자에서도 여성이 남성에 비해 ST elevation의 정도가 낮다
•
성별과 나이를 고려한 ECG criteria가 기존의 것보다 AMI에 대한 sensitivity와 specificity가 높음
A2. 남녀간 기저 ST segment의 amplitude와 AMI시 elevation 정도 차이 원인
•
여성이 myocardial mass가 더 적고 전기저항이 높은 mammary fat pad가 더 많아 precordial lead에서 특히 전압이 작게 기록될 수 있다
•
남성에서 ST level이 높은 것과 나이에 따른 변화는 testosterone level과 관련이 있다.
•
심전도상의 J point와 ST segment는 Ventricle의 action potential morphology 에서 Phase 1과 2에 의해 결정됩니다. Ventricle의 초기 재분극시 transmural voltage gradient를 결정하는 것은 Phase 1의 rapid K+ outward current인 Ito mediated spike-and-dome pattern이 얼마나 뚜렷한가 입니다. 이때 남성의 경우 epicardium의 Ito density가 높아 phase 1에서 notch가 크게 나타나며 phase 2에서 transmural voltage gradient가 높게 되고 이는 곧 J point와 ST level의 상승을 의미합니다. 동물실험에서 right ventricle의 Ito mediated phase 1 notch가 left ventricle에서보다 크다는 사실은 V5 lead(->LV) 보다 V2 lead(->RV) 에서 ST segment의 성별 차이가 뚜렷하게 나타나는 것을 설명하는 근거가 됩니다. 여기에 심방 및 심실에서 androgen receptor가 발견된다는 사실을 더해, testosterone이 정확한 기전은 모르지만 Ito density 를 매개로 심실 재분극에 영향을 주어 ST level의 성별 차이를 발생시키는 것으로 생각됩니다. 본 연구는 정상인을 대상으로 남성이 여성에 비해 J point 및 ST segment level이 높은 이유를 testosterone과 Ito density 에 근거하여 설명하고 있지만, 정상인이 아닌 STEMI 환자에서 성별에 따른 ST elevation 정도의 차이에 다른 기전이 있는지는 추가적인 연구가 필요할 것으로 생각됩니다.
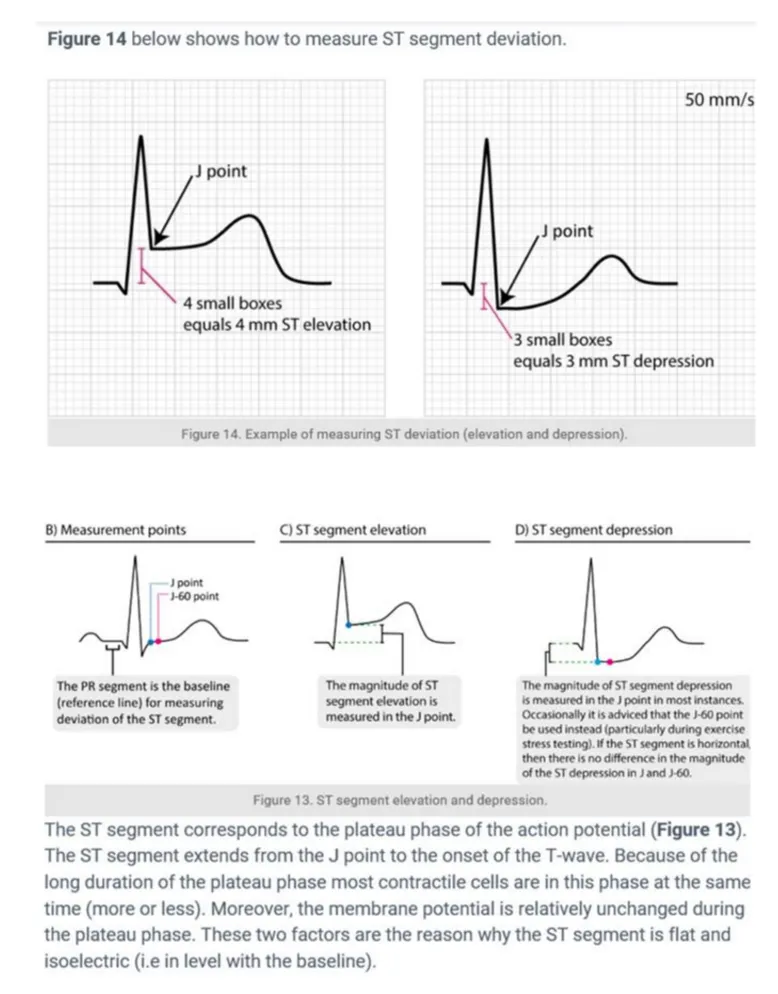
B. ST elevation의 측정
B1. J point
•
일종의 변곡점으로 QRS가 끝나고 ST segment가 시작되는 지점을 의미한다.
B2. Baseline
•
PR 분절의 upper edge에 해당되며, baseline과 J point의 upper edge 사이의 간격을 이용하여 STE을 측정한다.
B3. J point vs. J-60 or J-80 point
•
J point는 myocardium의 electral potential이 다른 경우 isoelectric하지 않기 때문에, 항상 ST segment deviation을 측정하는데에 적절하지는 않다. 이는 모든 ventricular myocardial cell이 동시에 탈분극이 완료되지 않기 때문에 일어나는 현상이다. 이를 보완하기 위해 J point의 60, 80ms 떨어진 지점인 J-60, J-80을 ST segment deviation의 판단 기준으로 사용하기도 하나, 현재의 가이드라인은 여전히 J point를 ST segment elevation의 기준으로 권장하고 있다.
C.ST elevation에서 acute STEMI가능성 높은 소견
1.
이전 EKG와 비교하여 새로운 ST segment의 변화 & dynamic change
2.
Reciprocal ST depression
3.
Ratio of T wave to QRS complex amplitude
•
T wave/QRS ratio < 0.36 in all precordial leads : LV aneurysm를 더 시사함
•
T wave/QRS ratio > 0.36 in any precordial leads : Anterior STEMI를 더 시사함
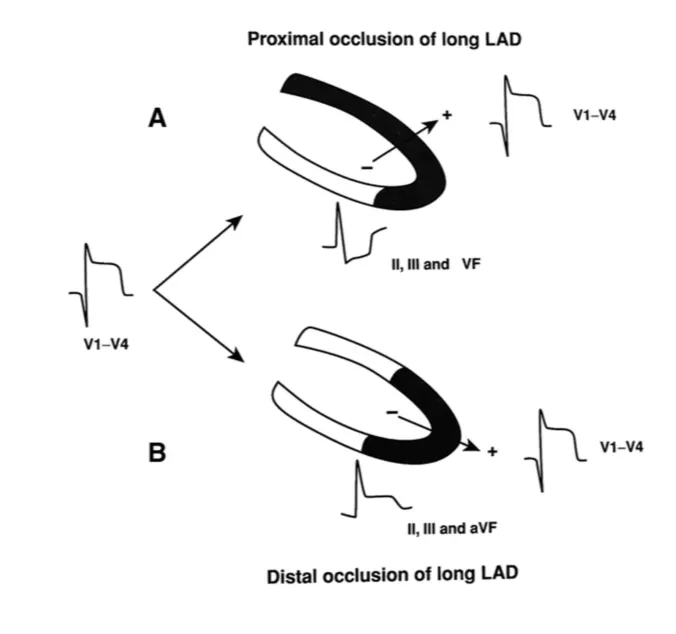
- Proximal 일 수록 손상 벡터는 앞쪽/위쪽을 향하므로, II, III, aVF에서 STD가 뚜렷하게 나타남.
- Distal 일 수록 STE이 나타나는 Lead의 개수는 오히려 증가한다.
- LAD 폐쇄 시에 경색 범위가 더 넓으므로, ST 변화가 더 뚜렷하다.
D. Lt main occlusion
•
손상벡터는 우측, 위쪽 (V1방향)
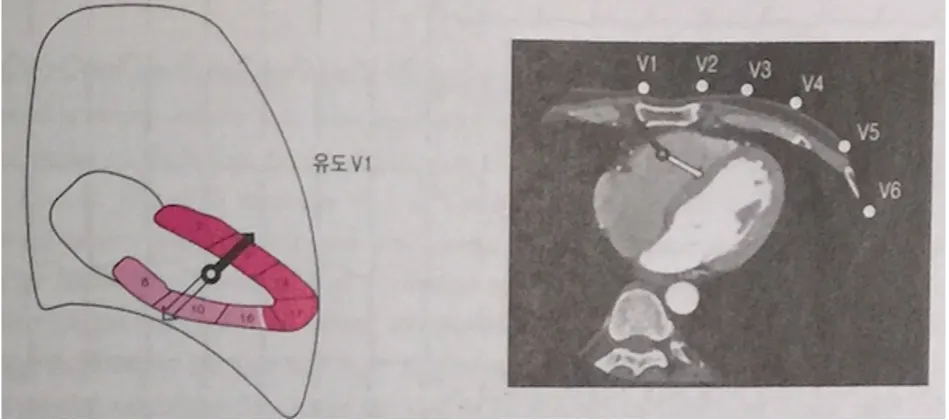
D1. 심전도 소견
•
광범위한 STD (특히 I, II, V4~6 에서)
•
aVR에서 1mm 이상의 STE
- ST 높이는 V1 ST 높이보다 더 높음.
- aVR STE는 3 vessel dz., ROSC, Shock, pLAD 경색 등에서도 보일 수 있음
•
V1에서 STE
- V2 에서의 STE는 LAD 경색때도 나타나지만 V1 STE은 Lt. main에서만 나타남.
•
나머지 흉부유도에서는 ST 변화가 LAD 경색 때보다 덜하다.
•
aVR, V1 을 제외하고는 STE 없는 경우 많다
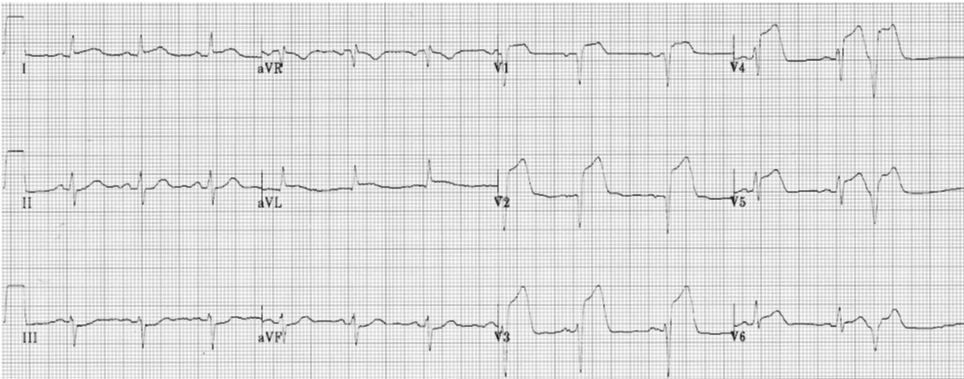
D2. aVR STE + infero-lateral reciprocal STD 사례
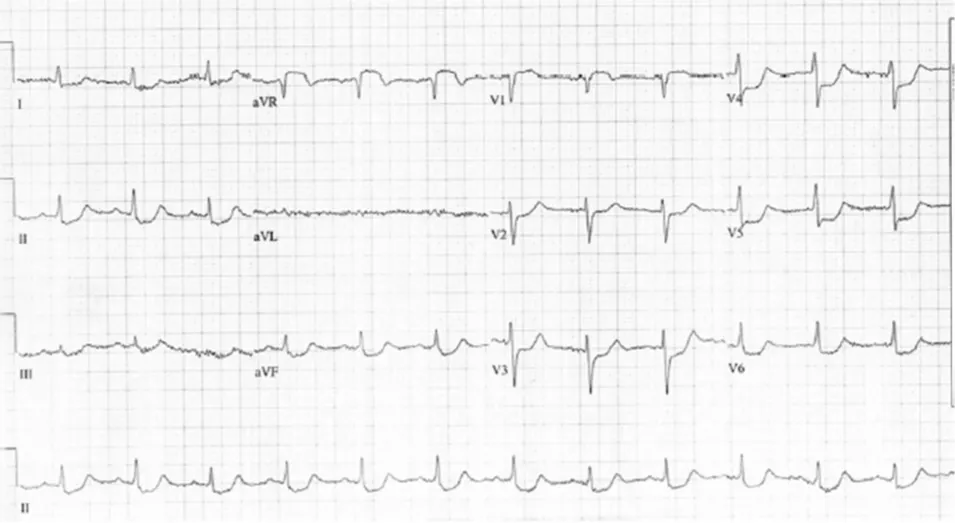
aVR, V1에서 STE 가 관찰됨
aVR STE > V1 STE
I,II, V4-6에서 STD가 관찰됨
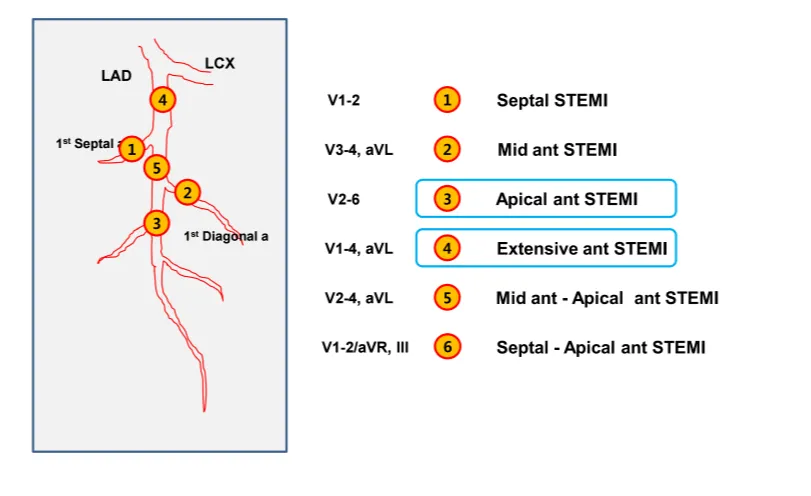
E. Proximal LAD occlusion
•
LAD의 LCX분지와 S1 사이 경색을 말한다 (D1이 S1보다 먼저 나오는 경우는 D1 전 까지)
•
손상벡터는 앞쪽, 위쪽을 향한다
•
광범위한 전벽, 전측벽 경색을 보인다
E.1. 심전도 소견
•
주로 V1-6 (± I and aVL) 중 연속된 2개 lead에서 STE with Q wave
40세 미만 남자는 2mm, 여자는 1.5mm 이상
•
inferior leads (mainly III and aVF)에서 Reciprocal STD.
•
aVR도 STE가 나타나나, Lt. main STEMI 때에 비해 높이가 낮다.
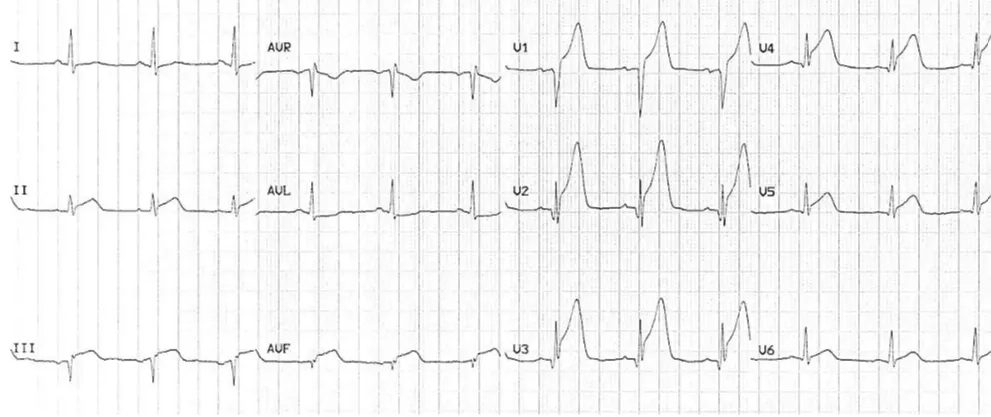
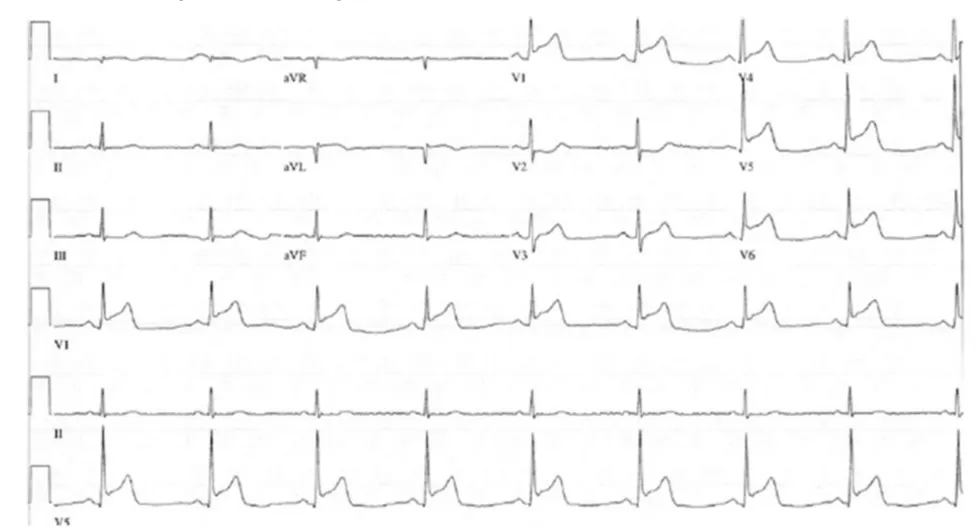
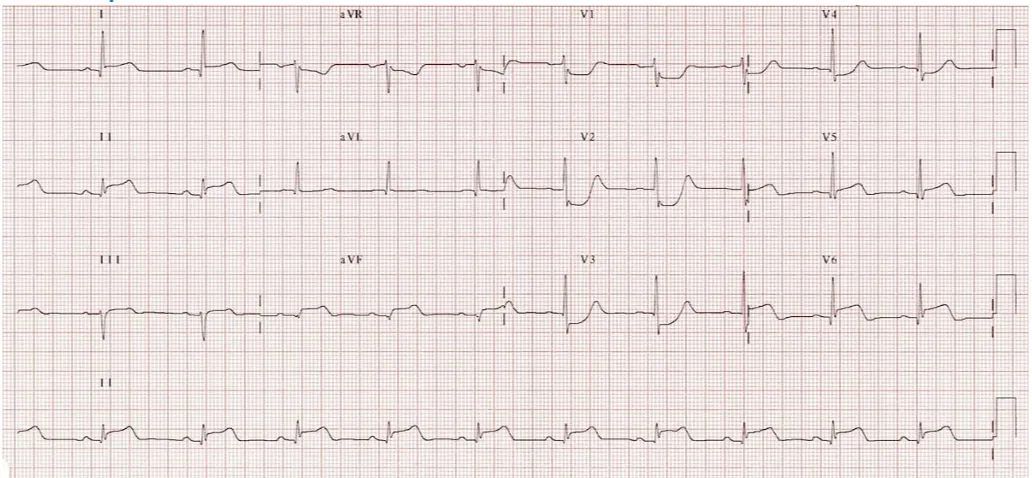
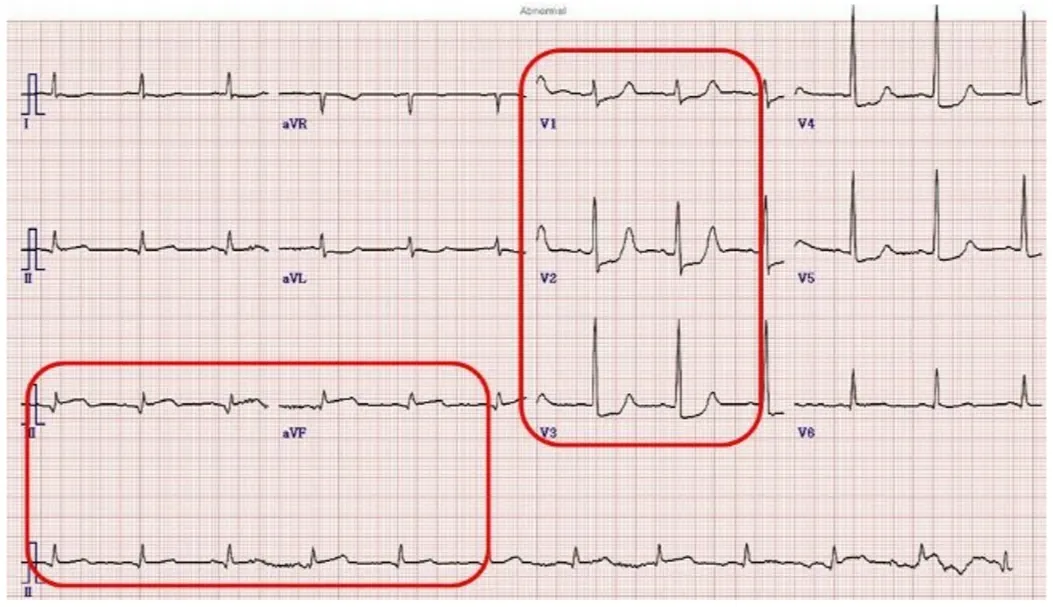
E2. Hyperacute Anteroseptal STEMI 사례
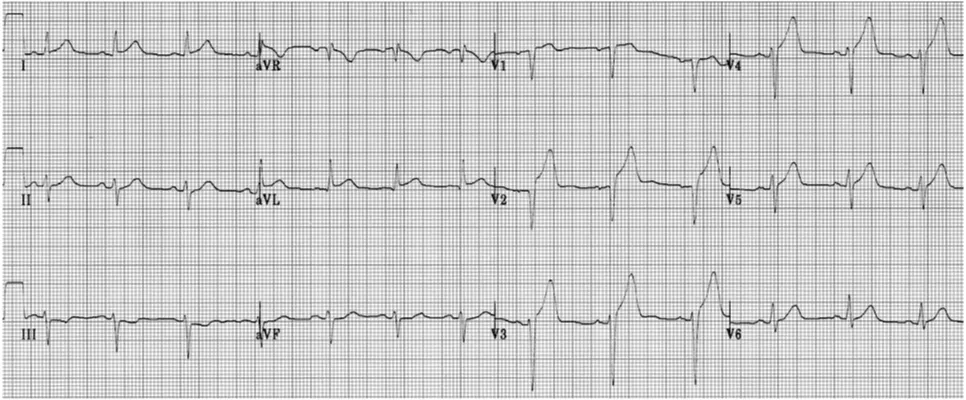
STE는 anteroseptal leads (V1-4) 에서 가장 높다
septal leads (V1-2)에서 Q 파가 나타난다
I, aVL and V5에 경미한 STE가 나타나며, III에서 reciprocal STD가 보인
V2-4에서 hyperacute T가 보인다
E3. Hyperacute Anterior STEMI 사례
V2-6에서 hyperacute T, R 파 높이가 낮아짐
APC, multifocal VPC : myocardium이 irritable 함을 의미 (VF 위험)
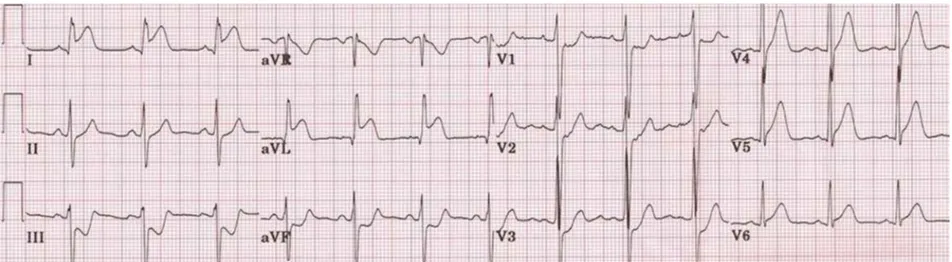
E4. Extensive Anterolateral STEMI (acute) 사례
STE 가 V2-6, I, aVL 유도에서 나타남
Reciprocal STD 가 III, AVF 유도에서 관찰됨
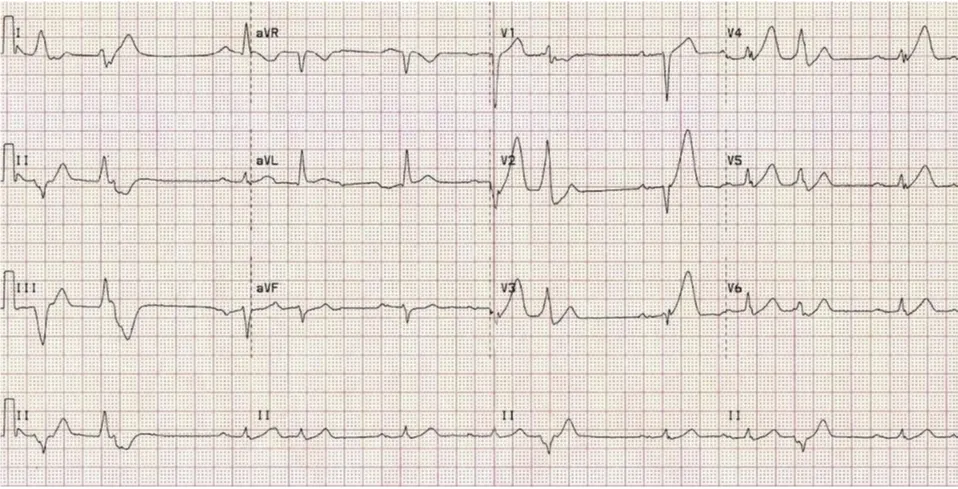
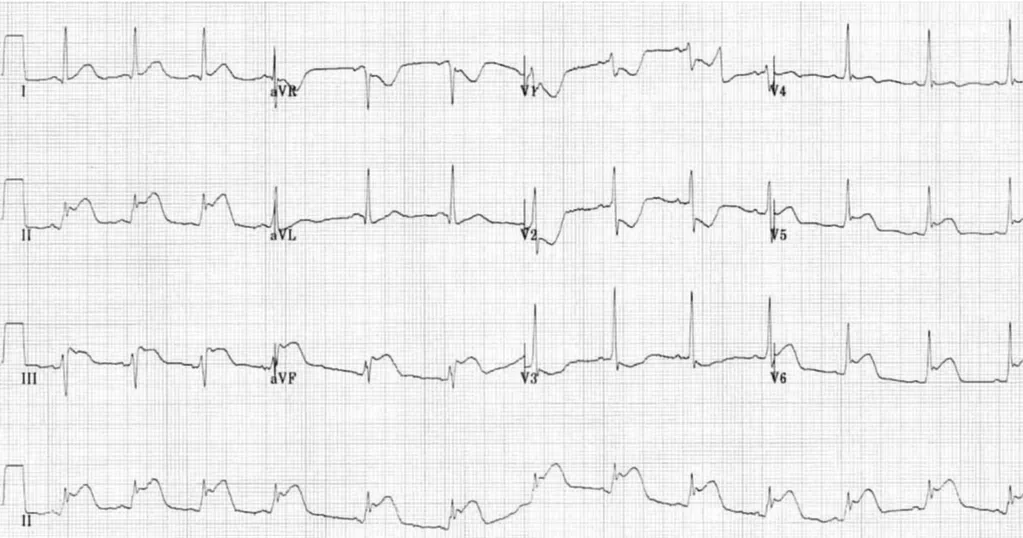
E5. Extensive Anterior STEMI (acute) 사례
ST elevation in V1-6 plus I and aVL (most marked in V2-4).
Minimal reciprocal ST depression in III and aVF.
Q waves in V1-2, reduced R wave height (a Q-wave equivalent) in V3-4.
There is a premature ventricular complex (PVC) with “R on T’ phenomenon at the end of the ECG; this puts the patient at risk for malignant ventricular arrhythmias.
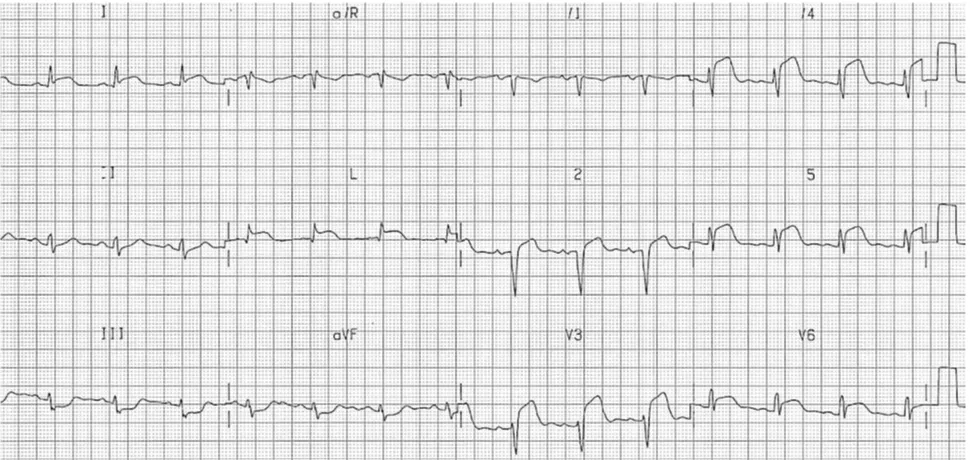
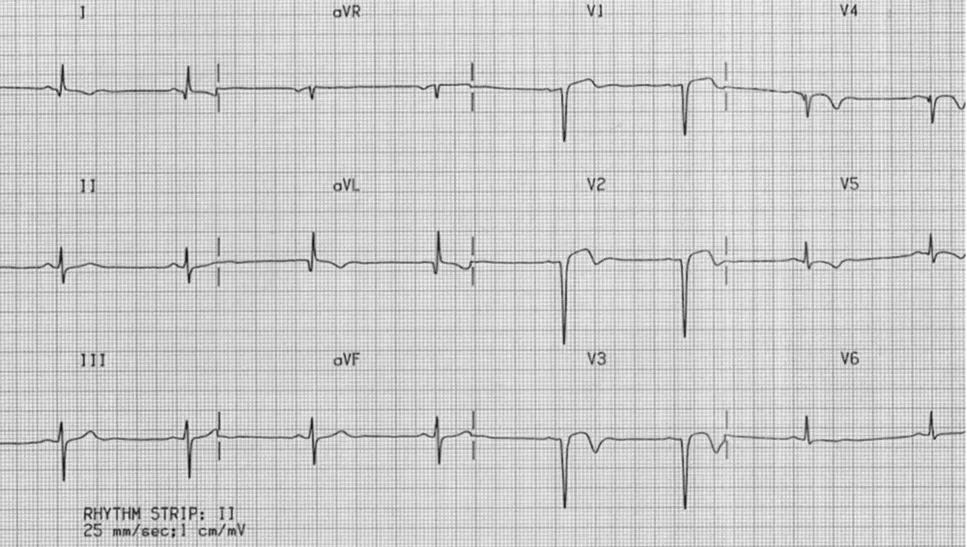
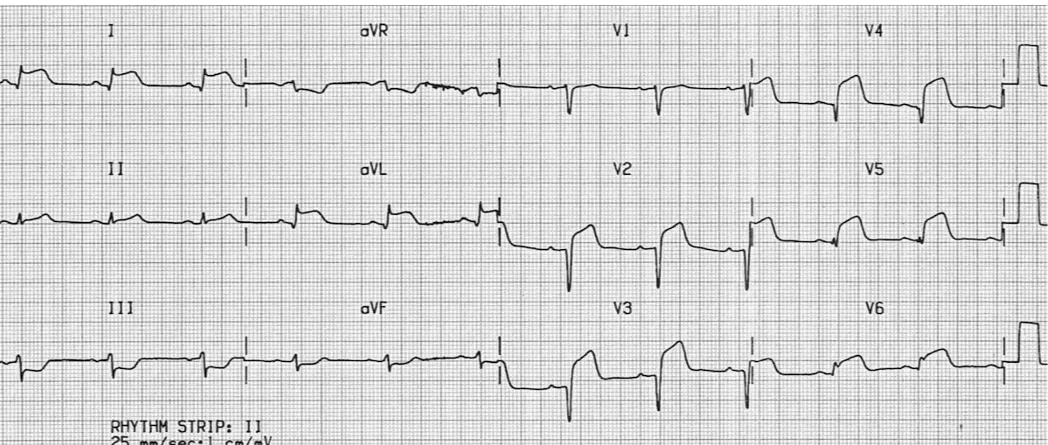
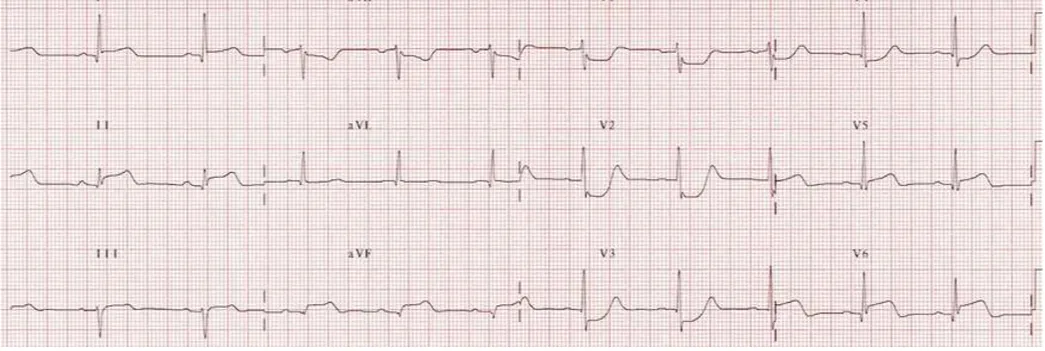
E6. Prior Anteroseptal / Lateral MI
•
Deep Q waves in V1-3 with markedly reduced R wave height in V4.
•
Residual ST elevation in V1-3 (“left ventricular aneurysm” morphology).
•
Biphasic/inverted T waves in V1-5.
•
Poor R wave progression (R wave height < 3mm in V3).
•
Abnormal Q waves and T-wave inversion in I and aVL.
•
The pattern indicates prior infarction of the anteroseptal and lateral walls.
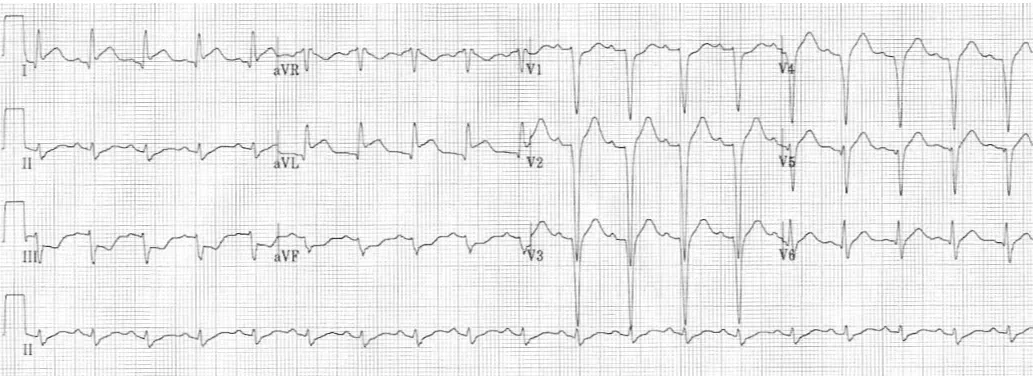
E7. massive anterior MI ("tombstoneing" pattern)
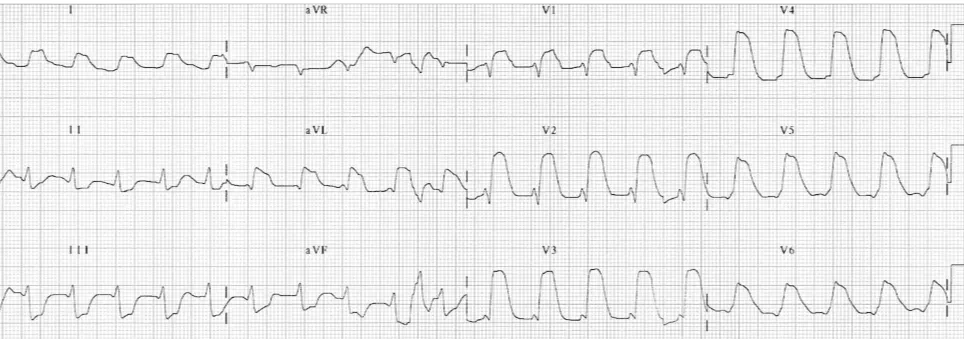
비석 모양같은 심한 STE 이 V1-6 와 high lateral leads (I, aVL) 에서 관찰됨
광범위한 경색과 LV EF의 저하 및 심인성 쇽, 사망의 위험성이 높다
E8. Anterior-inferior STEMI
•
STE이 전체 흉부유도와 하부유도에서 관찰됨
•
초급성 T파가 보이며, V1-3 유도에서 두드러짐
•
Q 파가 V1-3, III, aVF 유도에서 관찰됨
•
“type III” or “wraparound” LAD 경색인 경우 나타남
wrapaorund LAD : inferoanterior infarction
pLAD경색 시 LAD의 길이가 길어 inf wall 까지 나아간 경우는 하벽경색이 동반되면서 inf lead에서도 STE를 보임
inferoanterior STE pattern
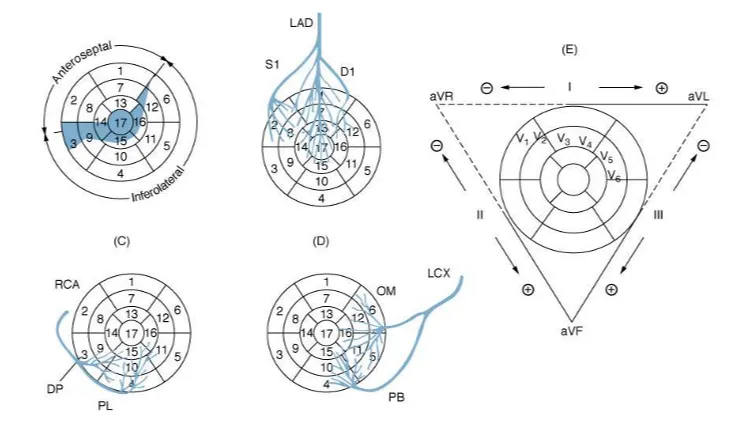
1. LAD Occlusion between S1 and D1 : mid
•
S1은 중격의 기저부, BB에 혈액공급 (aVR 과 V1 과 관련)
•
D1은 high lateral region에 혈액공급 ( I과 aVL 관련)
F.1. S1-D1 사이 occlusion
•
Septum 은 보존됨 (V1의 STE는 없음)
•
손상 벡터는 전방, 좌측(aVL)로 향함
•
aVL에 STE
•
STD ≥ 1 mm in II, III or aVF (reciprocal to STE in aVL)
F.2. D1-S1 사이 occlusion (D1이 S1보다 먼저 나오는 경우)
•
Septal-apical infarction
•
D1 영역은 Save됨.
•
손상 벡터는 우하방
•
V1-2/aVR, III 에서 STE
•
D1 영역이 살아있어, aVL은 STE없고, reciprocal change에 의해 STD만 나타남.
•
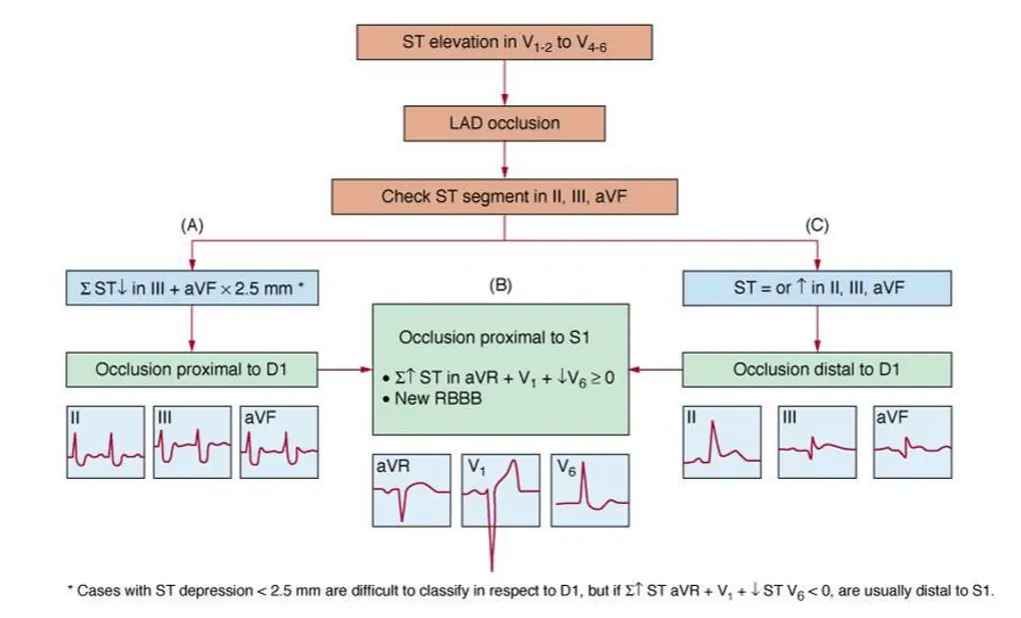
1. LAD Occlusion below S1 and D1: distal
•
Septum 은 보존됨 (V1의 STE는 없음)
•
손상벡터는 전방, 하방으로 향함
•
I, aVL, aVR의 STE는 나타나지 않음
•
II, III, aVF에 STE가 나타남
•
V3-6의 STE가 V2보다 더 뚜렷함
<Subtle Anterior STEMI Calculator>
심근경색 초반에는 경미한 변화만 생겨 자칫 심근경색 진단이 늦어질 수 있는데,
LAD 막힘으로 인한 심근경색 진단을 위해 4개의 변수를 고려한 공식이 개발된 바 있다.
네 개의 변수는 아래와 같다.
1.
Bazett-corrected QT interval in milliseconds,
2.
QRS amplitude in lead V2 in millimeters,
3.
R-wave amplitude in lead V4 in millimeters,
4.
ST-segment elevation 60 ms after the J point in lead V3 in millimeters.
아래 사이트에서 자동으로 계산이 가능한 것 같다.
컷오프 값은 18.2 인데, 이 때의 민감도는 89%, 특이도는 95%로 상당히 높다.
컷오프 값을 19.0으로 올리면 특이도가 97%까지 오르고,
컷오프 값을 17.0으로 낮추면 민감도가 97%가 된다.
1. Lateral STEMI
•
lateral wall은 LAD의 branch와 Lt. Circumflex 에 의해 공급
•
Lateral wall 경색은 anterolateral MI와 같이 광범위한 경색의 일부로서 주로 발생
•
Lateral wall 단독경색은 덜 흔하다
H.1. 심전도 소견
(1) I, aVL, V5-6에서 STE
(2) III, aVF에서 reciprocal STD
- I, aVL, V5-6에서 STE 있는 경우에만 보임
- inferolateral MI 인 경우에는 masking됨
참고
•
Anterolateral MI : LAD occlusion
•
Infero-posterior-Lateral MI : LCx occlusion
•
Isolated Lateral MI : D1, OM or ramus intermedius같은 작은 branch의 경색
H.2. Lateral STEMI (Lt. circumflex)
H.3. High Lateral STEMI --> Mid andterior STEMI
•
ST elevation is present in the high lateral leads (I and aVL).
•
There is also subtle ST elevation with hyperacute T waves in V5-6.
•
There is reciprocal ST depression in the inferior leads (III and aVF) with associated ST depression in V1-3 (which could represent anterior ischaemia or reciprocal change).
•
This pattern is consistent with an acute infarction localised to the superior portion of the lateral wall of the left ventricle (high lateral STEMI).
•
The culprit vessel in this case was an occluded first diagonal branch of the LAD.
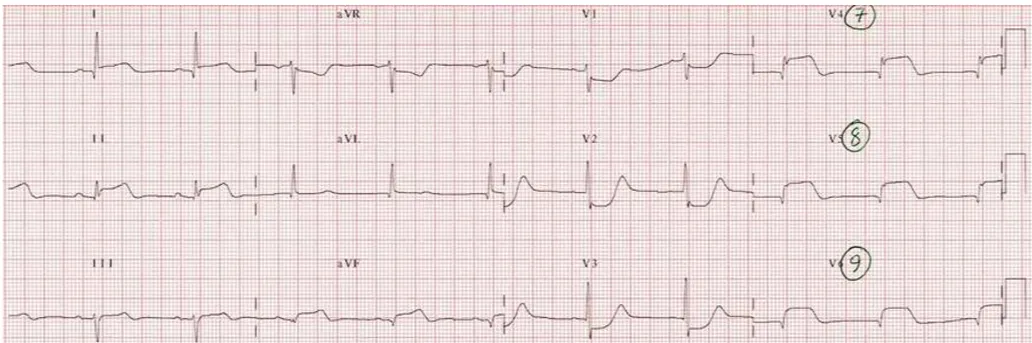
H.4. High Lateral STEMI:
•
ST elevation is present in the high lateral leads (I and aVL).
•
There is reciprocal ST depression in the inferior leads (III and aVF).
•
QS waves in the anteroseptal leads (V1-4) with poor R wave progression indicate prior anteroseptal infarction.
•
This pattern suggests proximal LAD disease with an acute occlusion of the first diagonal branch (D1).
H.5. Anterolateral STEMI:
•
ST elevation is present in the anterior (V2-4) and lateral leads (I, aVL, V5-6).
•
Q waves are present in both the anterior and lateral leads, most prominently in V2-4.
•
There is reciprocal ST depression in the inferior leads (III and aVF).
•
This pattern indicates an extensive infarction involving the anterior and lateral walls of the left ventricle
ST elevation in the precordial leads plus the high lateral leads (I and aVL) is strongly suggestive of an acute proximal LAD occlusion (this combination predicts a proximal LAD lesion 87% of the time).
H.6. Inferolateral STEMI:
•
There is ST elevation in the inferior (II, III, aVF) and lateral (I, V5-6) leads.
•
The precordial ST elevation extends out as far as V4, however the maximal STE is in V6.
•
ST depression in V1-3 is suggestive of associated posterior infarction (the R/S ratio > 1 in V2 is consistent with this).
•
•
This constellation of ECG abnormalities is typically produced by occlusion of the proximal circumflex artery.
H.7. Inferoposterolateral STEMI
•
STE : (II, III and aVF) and (I, V5-6).
•
STD : V1-3 with tall, broad R waves and upright T and a R/S ratio > 1 in V2 : 후벽경색 의미
•
The culprit vessel : pLCX
1.
inferior STEMI
•
전체 MI의 40-50%
•
전벽경색보다는 예후 좋음
•
하벽경색환자의 40%까지에서 RV infarct 동반
•
20%까지에서 서맥이나 AV block 동반
•
RCA/Lcx occlusion (RCA ~80%, Lcx 18%)
I.1. 심전도 소견
(1) II, III, aVF에서 STE
- II 보다 III에서 ST elevation이 강하게 나타나면 이는 RCA occlusion을 시사
(2) aVL (± I) 에서 reciprocal STD
•
aVL (± I) 에서 STD 보이면 RCA시사.
•
aVL(± I) 에서 STD 없으면 proximal LCX 의심
•
aVL(± I. V5-6) 에서 STE 보이면 proximal LCX 의심
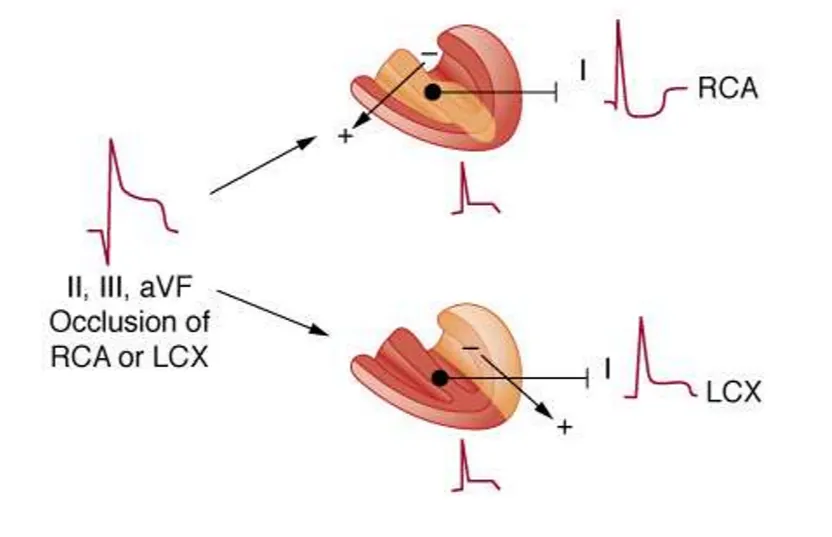
RCA

LCx
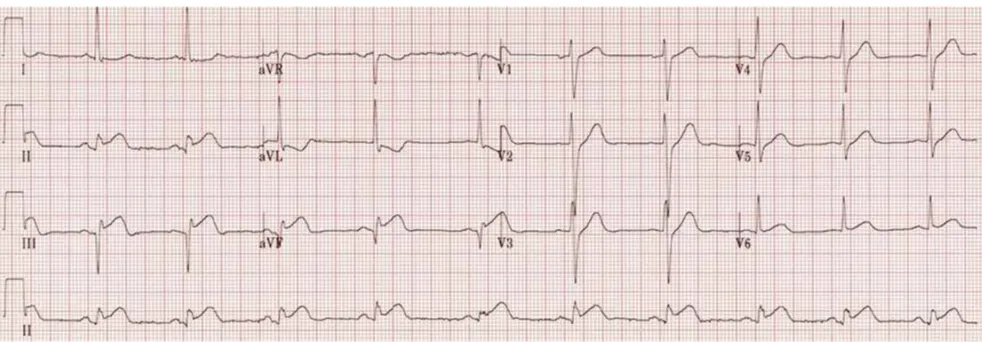
I.2. Early inferior STEMI:
•
Hyperacute (peaked) T waves in II, III and aVF with relative loss of R wave height.
•
Early ST elevation and Q-wave formation in lead III.
•
Reciprocal ST depression and T wave inversion in aVL.
•
ST elevation in lead III > lead II suggests an RCA occlusion; the subtle ST elevation in V4R would be consistent with this.
Note how the ST segment morphology in aVL is an exact mirror image of lead III. This reciprocal change occurs because these two leads are approximately opposite to one another (150 degrees apart).
The concept of reciprocal change can be further highlighted by taking lead aVL and inverting it… see how the ST morphology now looks identical to lead III.
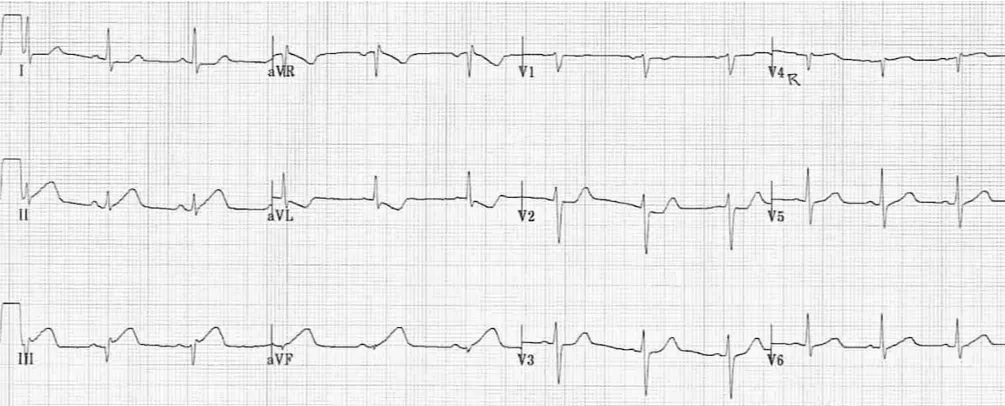
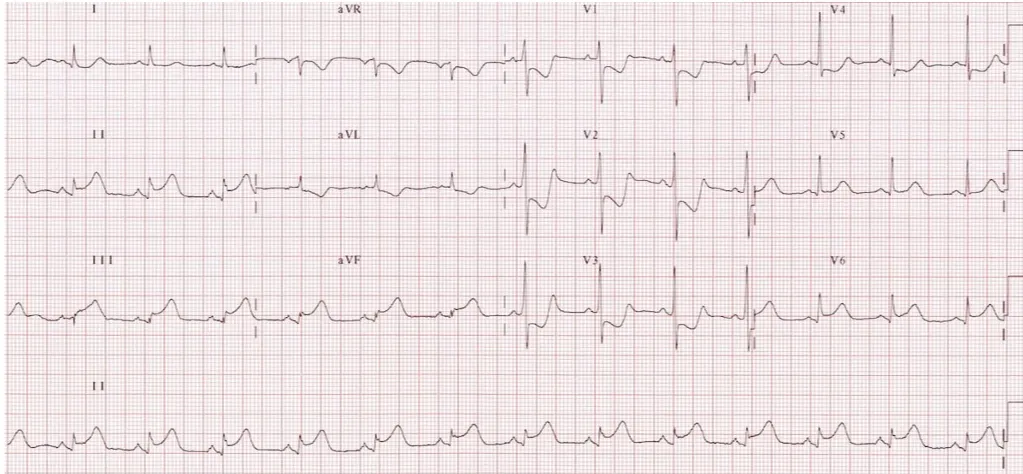
I.3. Massive inferolateral STEMI:
•
Marked ST elevation in II, III and aVF with a “tombstone” morphology.
•
Reciprocal change in aVL.
•
ST elevation is also present in the lateral leads V5-6, indicating an extensive infarct of the inferior and lateral walls.
In patients with inferior STEMI, ST elevation of 2mm or more in leads V5 and V6 is predictive of extensive coronary artery disease and a large area of infarction.
J.Posterior MI
•
AMI의 15~20%
•
보통 inf 또는 lateral infarc에 동반. 단독은 드물다
J.1. 심전도 소견
(1) V1-V3 에서
•
Horizontal STD
•
Tall, broad R (>30 msec)
•
Positive T wave
•
R/S ratio >0.5 in V1, V2(Q equivalent)
(2) Left dominant: STE (II, III, aVF/V5, V6)
(3) Non dominant: only STD (V1-V3)
J.2. Inferolateral STEMI. Posterior extension is suggested by:
•
Horizontal ST depression in V1-3
•
Tall, broad R waves (> 30ms) in V2-3
•
Dominant R wave (R/S ratio > 1) in V2
•
Upright T waves in V2-3
The same patient, with posterior leads recorded:
•
Marked ST elevation in V7-9 with Q-wave formation confirms involvement of the posterior wall, making this an inferior-lateral-posterior STEMI (= big territory infarct!).
J.3. Inferior STEMI with posterior extension. Extensive territory
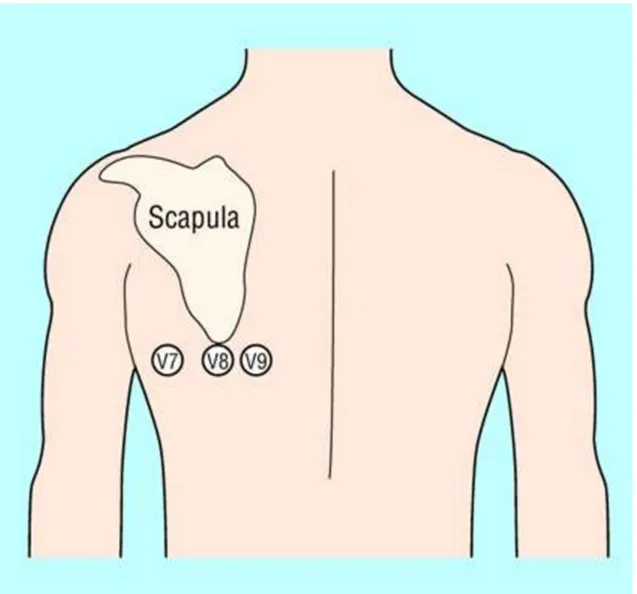
Leads V7-9 are placed on the posterior chest wall in the following positions.
•
V7 – Left posterior axillary line, in the same horizontal plane as V6.
•
V8 – Tip of the left scapula, in the same horizontal plane as V6.
•
V9 – Left paraspinal region, in the same horizontal plane as V6.
The degree of ST elevation seen in V7-9 is typically modest
– note that only 0.5 mm of ST elevation is required to make the diagnosis of posterior MI