


•
Pregnancy test
1.
Qualitative test : + (≥20mIU/mL in urine & ≥10mIU/mL in serum)
2.
Bedside urine test가 음성이라도 자궁외 임신을 배제할 수 없다.
3.
The sensitivity of quantitative serum test(≥5 mIU/mL도 detect가능)를 시행하여 확인이 필요할
수 있다.

A. Ectopic pregnancy
1, Pathophysiology
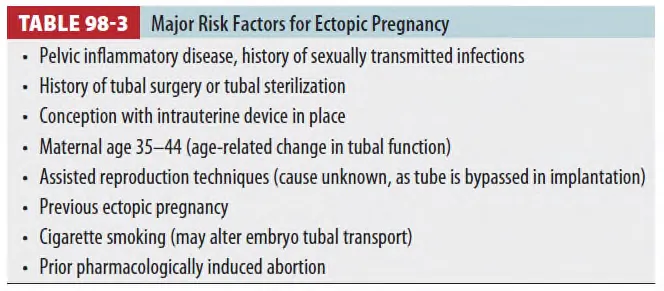
(1) The vast majority of ectopic pregnancies
: Fallopian tube, abdominal, cervical, cesarean scar ectopic pregnancy 등
2. History
(1) 자궁외 임신의 70%에서 amenorrhea가 고되지만,
No missed menses are reported in 15% of ectopic pregnancy cases.
(2) Prior tubal surgery를 받은 환자의 임신은 다른 것이 증명될 때까지 자궁 외 임신으로 간주한다.
(3) Vaginal spotting or bleeding (pain이 없더라도 비정상적인 질출혈은 자궁외임신 고려)
3.
Diagnosis
•
The diagnosis of pregnancy이 가장 우선이다.
•
The definitive diagnosis : US, Laparoscopy, Surgery
(1) Serum β-hCG
① The dynamics of β-hCG : 정상임신과 비정상임신에서 차이가 있다.
② 정상임신은 9~10주까지 빠르게 증가하나 비정상임신은 증가 속도가 느리며 감소할 수도 있다.
③ 단독으로 비정상임신을 확정할 수 없다.
④ Doubling time (β-hCG가 2배가 되는 시간)
: 정상임신의 경우 평균 2일
: 자궁외임신의 경우 절대적인 수치도 낮고 doubling time도 오래 걸린다.
•
정상임신은 49시간 내 β-hCG가 최소 53% 오른다. (평균 1일에 53%, 2일에 124%)
그러나 53% 이상 올랐다고 하여 비정상임신이나 자궁외임신을 배제할 수는 없다.
(2) Progesterone
① Progesterone이 낮으면 이는 임신 실패이거나 비정상임신의 가능성이 높다.
② Most pathologic pregnancies : ≤10nanograms/mL
≤5 nanograms/mL : nearly 100% pathologic (정상임신에서 ≤2.5는 고된 바 없다)
>25 nanograms/mL : 97% sensitivity for viable IUP
③ 그러나 아직 단독 또는 확진검사로 사용하면 안된다.
(3) US and Ectopic Pregnancy
① Transvaginal US scanning : IUP or an ectopic pregnancy의 초기진단에 도움
② Operator-dependent한 단점이 있다.
③ Transabdominal US를 우선 시행
(less invasive, wider field of view and easier orientation to pelvic organ)
→ 이상을 찾지 못하면 transvaginal US 시행 (better visualization of early pregnancy)
④ US에서 IUP를 확인하고 비정상임신이 이지 않으며 환자가 heterotopic pregnancy의 risk가
없다면 자궁외임신을 배제할 수 있다.
(Heterotopic pregnancy : 정상임신과 비정상임신이 동시에 되는 것, 불임치료 받은 사람에게 잘 발생)

(4) The Discriminatory Zone
정의 초음파에서 ① : 정상임신이 일 것으로 생각되는 β-hCG level
② 초음파를 이용하여 정상임신도 비정상임신도 확인이 되지 않았을 경우 고려할 방법으로 환자의
β-hCG가 Discriminatory Zone다 높으나 empty uterus인 경우 자궁외임신을 의심.
(1500mIU/mL - 질식초음파, 6000mIU/mL - 복부초음파)
•
Equivocal case에서 영상전문의에게 협진을 요청하고 β-hCG가 낮아도 자궁외임신이 의심되는 경우
반드시 초음파를 시행하여야 한다.
(5) Other Diagnostic Modalities
① MRI : High sensitivity & specificity, but cost, availability, and the time to perform
② Culdocentesis
: 초음파 대신 사용. 검사양성일 경우 surgical intervention 고려.
: Dry aspiration은 진단적 의미 없음.
: Clear하고 non-bloody → Negative / Nonclotting blood constitutes → Positive
: No consensus regarding the criteria for a positive test
: 대부분은 rupture에서 +이나 unrupture에서도 + 나올 수 있음
③ Laparoscopy : both diagnostic and therapeutic, but invasive
4.
Treatment
(1) Surgical or medical
① V/S stable & Unrupture : Surgical - Laparoscopic salpingostomy
(MTX, salpingotomy, and salpingectomy 치료 차이 없음)
② V/S unstable : Laparotomy
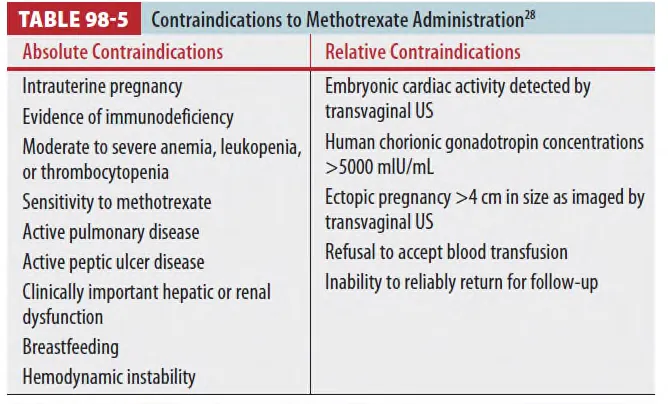
(2) Methotrexate(MTX) : Only drug
① 혈역학적으로 안정, 통이 심하지 않고, 간이나 신장의 기능에 이상이 없는 경우 사용
② IM(더 선호됨) or G-sac에 직접주입 모두 가능
③ Side effect : 통 (가장 흔함), 일반적으로 그냥 호전되나 필요 시 진통제 사용
④ V/S이 불안정하거나 lab 상 출혈이 의심되면 surgical intervention 고려해야 한다.
(3) Rh Seroconversion and Indications for Anti-D Immunoglobulin
① Rh O (D) antigen은 임신 5.5~6주 사이에 발견된다.
② 0.1ml의 태아의 피만 모체와 섞여도 발생한다.
③ 임신 12주 이전 진단
: Treatment with 50micrograms of RhoGAM for Rh-negative women with ectopic
pregnancy (Full dose of 300micrograms is acceptable as well)
•
Diagnostic algorithm for suspected ectopic pregnancy

B. Emergencies in the First 20 Weeks of Pregnancy
•
Common Causes of Vaginal Bleeding During the First Trimester of Pregnancy :
Abortion, Ectopic pregnancy, Gestational trophoblastic disease,
Implantation bleeding (physiologic)
1.
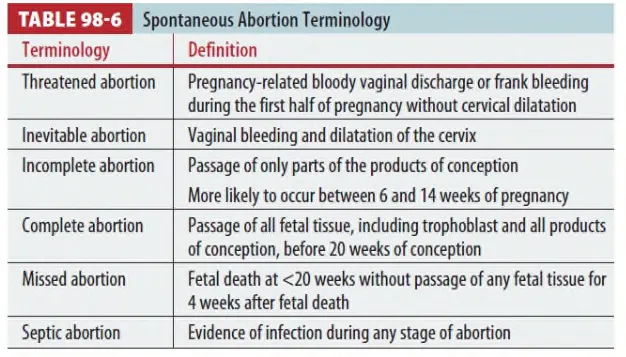
Spontaneous abortion
(1) 20주 미만 또는 500g 미만의 태아를 잃는 것으로 정의됨
(2) 주 증상 : Bleeding with or without abdominal pain
(3) 진단 : serum β-hCG level check, lab test, US
(4) 치료
① Threatened abortion : Discharge & bed rest 권고
② Incomplete abortion
: 치료 필요 – Medication (PO misoprostol, 600micrograms) or Surgical (D&C)
③ Complete abortion
: Discharge & f/u, 확실치 않으면 산부인과 협진
④ Fetus가 안 이면 입원 또는 1주 뒤 f/u, 출혈이나 증상이 심하면 입원
⑤ 임신이면서 vaginal bleeding 있고 Rh-negative이면 RhoGAM 치료

2.
Septic abortion
(1) Spontaneous or other abortion complicated by a pelvic infection
(2) 검사하고 IV antibiotics, hydration, 산부인과 consult
3.
Gestational trophoblastic disease
(1) Broad spectrum of conditions
(2) Uncomplicated partial hydatidiform molar pregnancy ~ Stage IV choriocarcinoma with
cerebral metastases
(3) 증상
① Vaginal bleeding
② Hyperemesis
③ 임신 second trimester까지 유지되면 pre-eclampsia 유발 가능
(24주 이전에 임신성 고혈압 발생 시 의심)
(4) 비정상적인 β-hCG level, 자궁의 크기가 주수와 맞지 않고, US 상 의심 시 협진
(5) 치료 : Suction curettage, β-hCG이 감소하지 않으며 chemotherapy 고려
4.
Implantation bleeding
5.
Nausea and vomiting, Hyperemesis gravidarum
(1) 12주 이전에 잘 나타남
(2) N/V 증상이 volume depletion 없이 나타는 경우는 정상적이나, 통이 동반되거나,
Hyperemesis gravidarum은 발생하는 것은 일반적이지 않다. 다른 질환 감별이 필요하다.
(3) 치료 : Hydration

