
•
Critical limb ischemia: blood flow 의 제한으로 인해 pain at rest, ulceration, gangrene이 발생.
•
Peripheral arterial disease : An ankle-brachial index < 0.9
I. Epidemiology
1.
위험요인
(1) Smoking, DM : M/I
(2) Other Risk factor : HTN, Hyperlipidemia, Hyperhomocysteinemia, elevated CRP
(3) SES 낮은 국가에서 유병률 더 높음.
2.
동반질환
(1) Myocardial infarction
(2) Ischemic stroke
(3) Death from vascular disease
3.
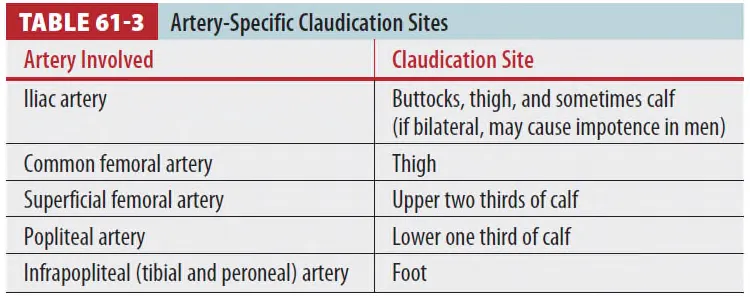
호발 동맥 : Femoropopliteal > Tibial > Aortoiliac > Brachiocephalic vessels
4.
Mortality : 1 year mortality 25%, Survivors의 1/4 이상이 amputation
Ⅱ. Pathophysiology
1.
Lack of blood supply
(1) Collateral vessel이 없으면, peripheral n. & skeletal m.이 먼저 비가역적 변화 (4~6시간 내)
2.
Reperfusion injury
(1) Compartment syndrome, rhabdomyolysis, metabolic derangements 등의 양상으로 나타남.
(2) Hyperkalemia, myoglobinemia, metabolic acidosis와 같은 합병증이 발생하며
arterial occlusion 으로 인한 사망의 1/3정도가 reperfusion injury의 합병증으로 사망.
3.
Thrombotic occlusion(m/c)
(1) >80% in lower limbs, 50% in upper limbs
(2) Atherosclerosis, gradually (due to collateral vasculature)
4.
Embolic occlusion : 1/3 in upper limbs
(1) Cardiac origin (m/c) : AF > Mural thrombus in the ventricle after recent MI
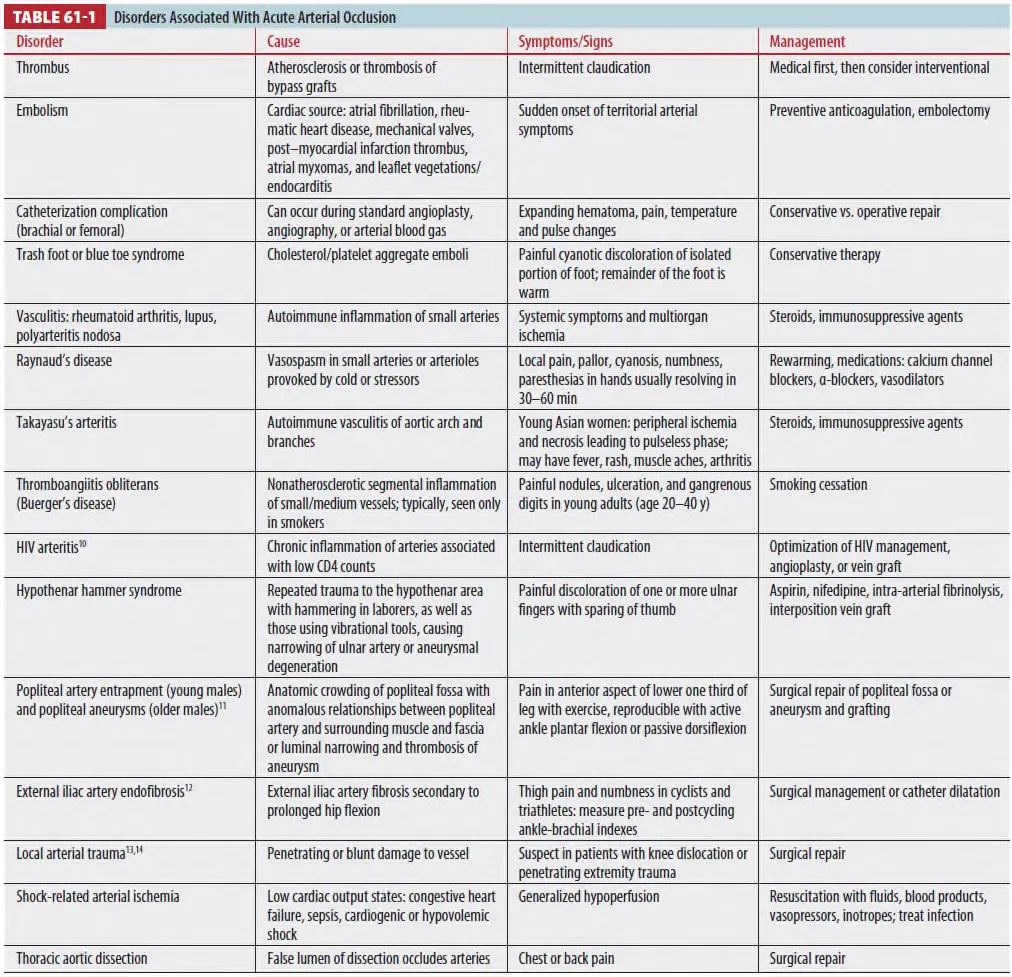
(2) Non-cardiac origin
① Aneurysm, atheromatous plaques에서 혈전이 생성되고 plaques가 부서지면서 미세순환을 폐쇄
② 이후 손, 발(Blue toe syndrome) 또는 TIA와 같은 증상이 다발성으로 발생할 수 있다.
(3) Other causes
① Intra-arterial drug injection
② Arterial ischemia d/t prolonged use of vasopressor
③ Aortic dissection
(4) 호발 위치-다리는 bifurcation of the common femoral a > popliteal a 팔은 brachial a
Ⅲ. Clinical features
1.
“Six Ps”
(1) Pain (earliest Sx.) (2) Pallor (3) Paralysis
(4) Pulselessness (5) Paresthesia (6) Poikilothermia
2.
피부 변화
(1) Pallor → Blotchy/mottled areas of cyanosis → Petechiae/blisters → Skin and fat necrosis
3.
Tissue viability
(1) Preservation of light touch → Good guide to tissue viability
(2) Muscle paralysis, sensory loss, prolonged ischemia → Nonviable
4.
Acute (2주 이내) vs Chronic arterial disease
(1) Acute limb ischemia의 pain
① Pain waking the patient at night
② Requiring the patient to hang his or her feet over the bed
③ Not relieved by rest or gravity, not well localized
(2) Chronic obstructive arterial disease의 pain
① Intermittent claudication, 진행되면 intermittent ischemic pain at rest
•
Claudication : cramp-like pain, 운동 시 악화되고 휴식 시 호전되는 통증
5.
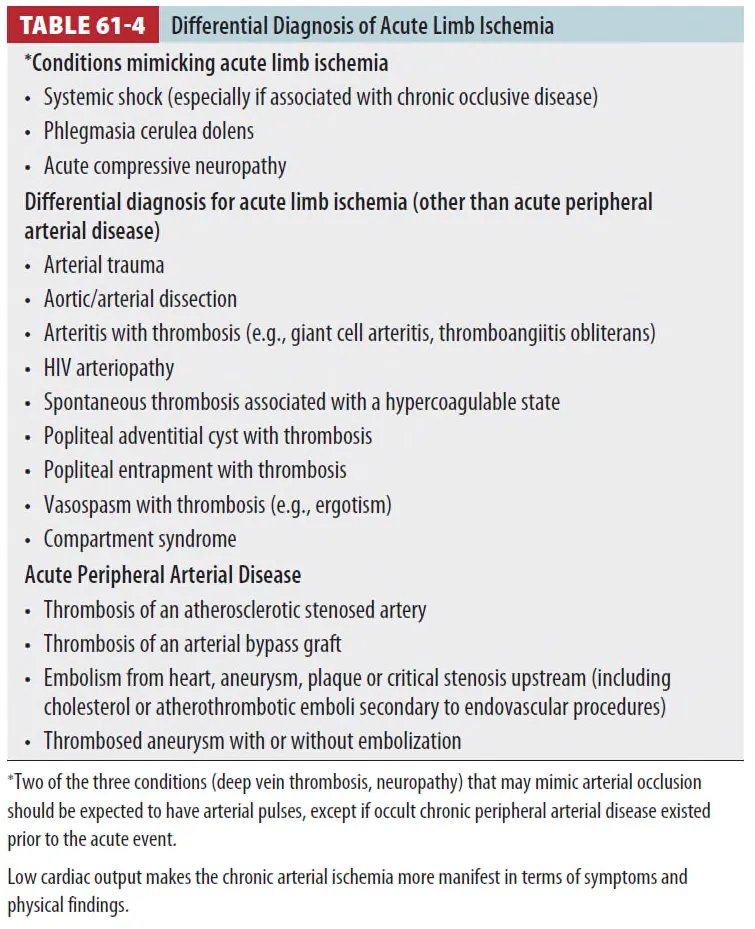
유사 증상을 나타내는 질환
(1) Acute limb ischemia를 DDx하는 3단계
① Look for conditions mimicking acute limb ischemia.
② Consider non-atherosclerotic causes of arterial occlusion.
③ If neither of the above exists, determine if the ischemia is caused by an thrombus or
embolus
Ⅳ. Diagnosis
1.
History
(1) Focus on the timing and acuity of symptom onset,
(2) Pattern of claudication
(3) past medical Hx
(4) Embolism vs Thrombosis

2.
Physical exam
(1) Look at the skin
(2) Palpate peripheral pulses(both)
(3) Seeking bruits and murmurs
(4) Chronic
① Shiny ② Hyperpigmented skin with hair loss and ulceration
③ Muscle atrophy ④ Poor pulses
(5) Hand-held Doppler US : 혈류의 유무, 강도를 확인
(6) Doppler로 혈류를 확인했으면 ABI를 측정 (위험도 평가)
① > 1.3 : Noncompressible
② 0.91~1.3 : Normal
③ 0.41~0.90 : Chronic peripheral a. disease
④ <0.40 : Severe
3.
혈액검사
(1) CPK, myoglobin, serum lactate (2) Electrolyte, glucose
(3) BUN, Cr, U/A (4) CBC
(5) PT, aPTT (6) Cardiac marker
4.
영상검사
(1) Time sensitive diagnosis : 의심되면 영상학적 진단 전에 먼저 surgical consult를 한다.
(2) 적절한 검사법을 선택하기 위해 EM, 혈관외과, intervention radiologist가 함께 결정해야 한다.
① Duplex US
: Very accurate for detecting complete or incomplete obstruction
: 하지만 calf level 아래쪽에서는 localization의 sensitivity가 감소한다.
② POCUS : Aorta, iliac vessels, femoral artery bifurcation 확인 가능.
③ TTE : Embolic sources를 확인 가능 / TEE: Aortic root pathology를 확인 가능.
④ Arteriography : Direct therapy 전에 OR, intervention lab에서 시행
⑤ CT with contrast : 응급실에서 바로 가능, large vessel에서는 arteriography와 Sn 유사.
⑥ MRI : CTA보다 Sn, Sp 높으나 less available
Ⅴ. Treatment
1.
목적
(1) Restoration of blood flow
(2) Preservation of limb and life
(3) Prevention of recurrent thrombosis or embolism
2.
Medical treatment
(1) IV unfractionated heparin (m/c initial tx)
(Heparin-induced thrombocytopenia에서는 direct thrombin inhibitor - Lepirudin, Argatroban)

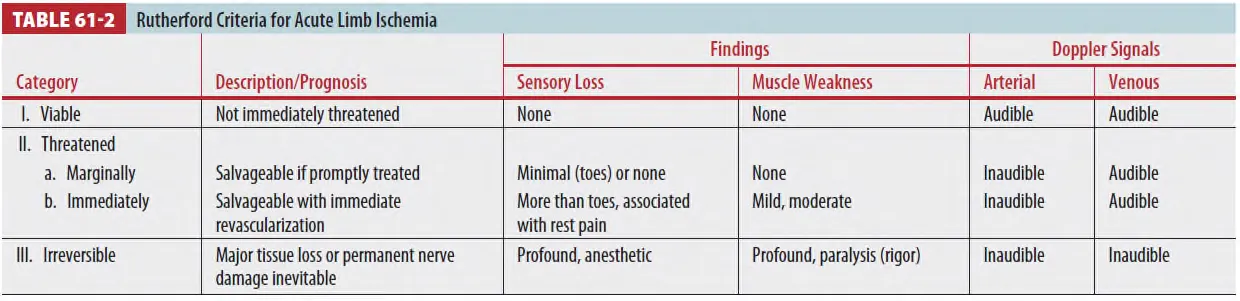
(2) Rutherford criteria stage에 따른 치료
① Stage I, stage IIa : 진단을 위해 영상학적 검사가 우선
② Stage IIb : 검사보다 즉각적 revascularization이 필요
③ Stage III : 이미 irreversible damage를 입은 상태, Amputation을 시행
3. Definitive treatment
(1) Catheter-directed thrombolysis
(2) Percutaneous mechanical thrombectomy
(3) Revision of an occluded bypass graft
(4) Revascularization with either PTA or standard surgery
4.
Long term non-surgical management
(1) 금연, 운동, 약물치료
(2) 항혈전제 (Aspirin : 75-100mg/d or Clopidogrel : 75mg/d)
① Reduce mortality from CVD with PAD
② Dual antiplatelet therapy 는 처음부터 추천하진 않음.
(3) ‘ACC/AHA 2016 guideline’
① Cilostazol(PDEi)를 intermittent claudication의 치료에 class I으로 추천
② Pentoxifylline은 사용하지 않는다.
(4) 다학제적 접근(전문의, 상처치료사, 영양사)이 morbidity를 줄이고 long term outcome을 개선
Ⅵ. Special consideration
1.
Upper extremity ischemia
(1) Much less common : Collateral circulation이 많아서 (허혈 자체도 적고 관련 합병증도 적다)
(2) Causes
① Vasospasm ② Arteritis ③ Trauma
④ Atherosclerotic plaque rupture ⑤ Embolism
⑥ Iatrogenic injury (e.g., during brachial artery access for cardiac catheterization)
⑦ Thoracic outlet syndromes ⑧ Aneurysms ⑨ Hypercoagulable states
(3) Diagnosis : 이외 PAD와 같은 방식
(4) Treatment : Heparin and emergent surgical thromboembolectomy
