
I. Introduction
1. Cardiomyopathy
(1) 심구조의 직접적인 변화, 심근 기능의 장애, 또는 심근의 전기적 특성을 변화시키는 여러 질환을 총칭
(2) 최근에는 molecular genetics and description of (ion) channelopathies의 연구가
cadiomyopathy에 대한 definition과 classification을 revision 하고 있음.
(3) 가장 최근 proposed 된 것은 MOGE(S) classification
1 Morphofunctional phenotype (M)
2 Organ involvement (O)
3 Genetic inheritance pattern (G)
4 Etiology (E: which includes genetic defect or underlying disease)
5 Functional status (S)
(4) 다만 simple terms으로의 cardiomyopathy를 아래에서 다룰 것이다.
2. Primary cardiomyopathy
(1) 대부분 myocardium만을 involve하며, 유전적인 요인으로 생기는 경우가 많음.
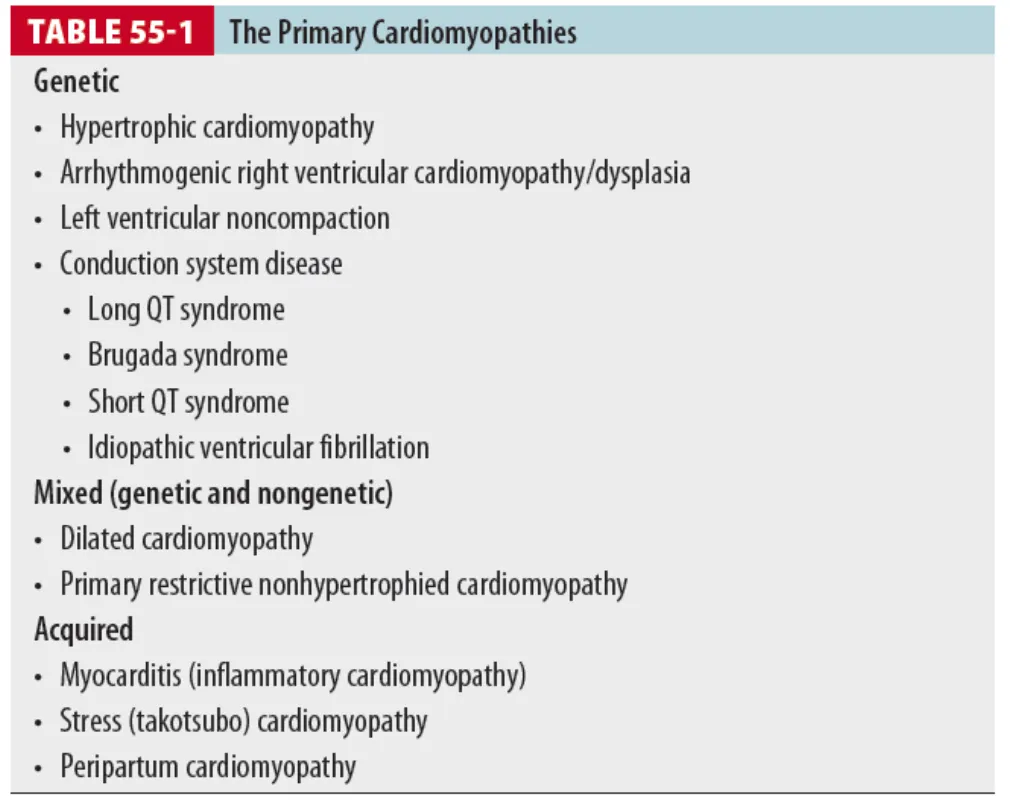
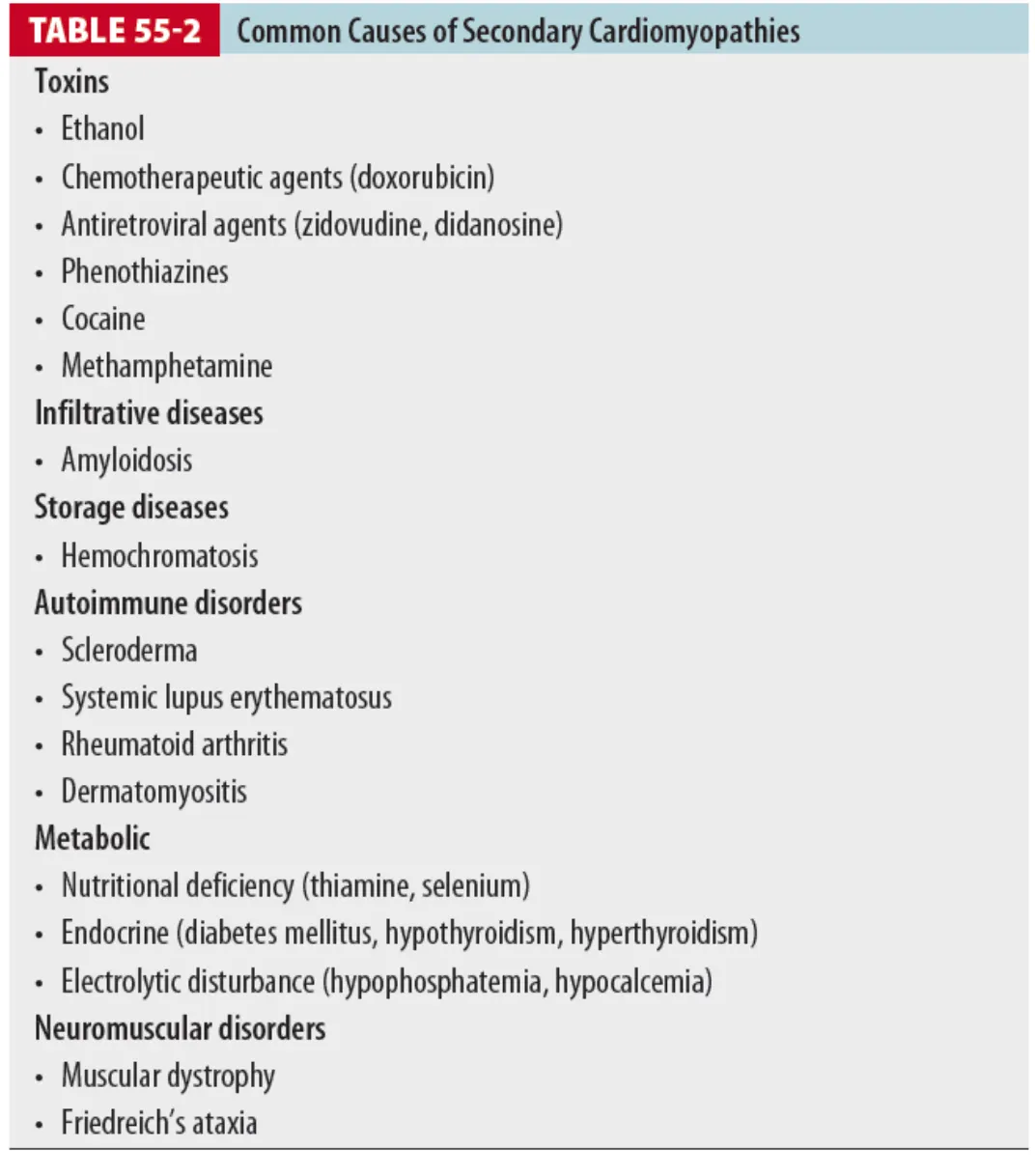
3. Secondary cardiomyopathy
(1) 특정 전신 질환과 연관된 심근병이 포함
(2) 주로 morphofunctional phenotype과 연관
(3) Idiopathic dilated or restrictive 형태의 cardiomyopathy와 비슷한 혈역학적 특성을 보인다.
(4) 심근병증은 미국 심장병 중 관상동맥(허혈성) 심장병, 고혈압성 심장병에 이어서 3번째로 흔한 질환
(5) 비후성 심근병증은 사춘기 인구의 sudden cardiac death의 두 번째 흔한 원인이며,
운동선수의 가장 흔한 sudden death의 원인이다.
구로고려대 김현진
•
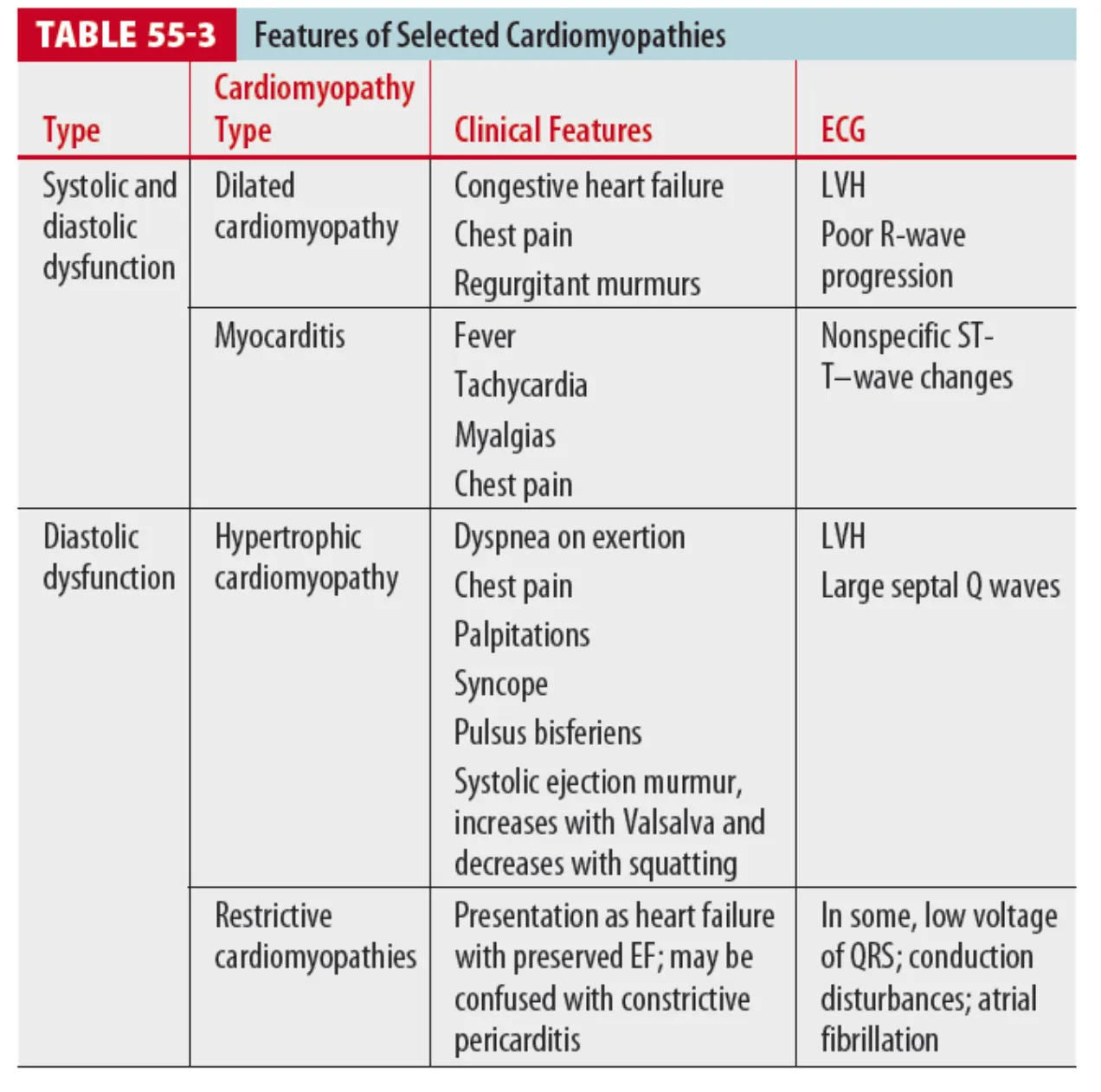
모든 Cardiomyopathy에 대하여 다룰 수 없기 때문에, 위의 table 55-3에 소개된 cardiomyopathy에
대해 다룰 것이라고 함.
•

B. Cardiomyopathies with systolic and diastolic dysfunction
B1. Dilated cardiomyopathy
(1) Epidemiology and pathophysiology
1 Dilated cardiomyopathy라는 term은 어떤 single disease를 의미하는 것이 아니며,
다만 non-specific한 phenotype으로 이해해야 함.
2 유전적인 요인이나 specific한 cardiac or system disorder와 함께 일어날 수 있음.
3 가장 흔한 예로 peripartum cardiomyoapthy가 있음.
4 Heart failure의 major cause이며 대부분의 환자들이 20~50대에 진단.
(2) Clinical features
1 Systolic pump failure로 인해 CHF의 증상 (DOE, orthopnea, paroxysmal nocturnal dyspnea,
bibasilar rale, dependent edema)을 보인다.
2 저하된 심실의 수축력과 심실확장은 mural thrombi 형성을 일으켜 peripheral embolization의
증상 (acute neurologic deficit, flank pain, hematuria, pulseless, cyanotic extremity) 보임
3 흉통은 제한된 coronary vascular reserve에 의해 발생 가능함.
(즉 atherosclerotic coronary artery disease 와는 pathologic하게 다른 형태로)
4 Murmur
: Holosystoclic mitral, tricuspid regurgitant murmur가 apex나 left lower sternal border에서
들린다 (Annular dilatation & Papillary m. displacement → Atrioventricular valve 불완전 닫힘)
: Apical diatstolic rumble이 들릴 수 있다.
(3) Diagnosis
•
Echo와 individual하게 맞춰진 testing을 통해 정해짐.
1 Chest radiograph
: Enlarged cardiac silhouette과 increased CT ratio를 보인다.
: Pulmonary hypertension의 증거(cephalization)를 보인다.
2 ECG
: 거의 항상 비정상으로 보이며 LV hypertrophy와 left atrial enlargement가 가장 흔한 소견이다.
: Q or QS wave와 poor R progression이 anterior precordium에 보일 수 있다.
(Pseudo-infarction pattern)
: Atrial fibrillation과 ventricular ectopy가 흔한 리듬 장애이다.
3 Echocardiography
: Decreased EF
: Increased systolic and diastolic volume
: Ventricular and atrial enlargement를 보인다.
(4) Treatment and disposition
1 급성치료는 acute decompensated heart failure와 같다.
2 만성치료로 diuretics, digoxin을 사용할 수 있지만 생존율을 개선하지는 못한다.
3 ACEi, β-blocker (carvedilol)은 dilated cardiomyopathy와 CHF의 생존율을 개선한다.
4 응급실로 내원한 환자의 원인이 noncompliance 할 경우 nitrates, IV diuretics, reinstitution of
prescribed medication, patient counseling, primary care physician으로 refer 하는 것이 적절
: 하지만 life-threatening cause(cardiac ischemia)에 대해서 우선적으로 고려해야 한다.
: 급성으로 증상이 있는 환자에 있어서는 입원하여 definite diagnosis와 management를 해야 한다.
5 Heart transplantation을 기다리거나 destination therapy로 LV assist device를 사용하는 경우도
있다.
•
-------------------------------------------------------------------
* Left Ventricular assist devices (LVADs)
1. LVAD는 end-stage heart failure 환자에서 transplantation을 기다리거나 또는 그 destination
therapy로 사용되어 왔다. 많은 모델이 있으나 similar한 feature를 공유한다.
2. LVAD는 implanted pump가 LV의 apex로부터 proximal aorta까지 피를 transfer 시킨다.
(1) Pump는 external power source가 있고, controller와 연결되어 있다.
(2) 배터리와 컨트롤러는 환자가 같이 들고 다닐 수 있다.
(3) Surgical incision을 통해 pump와 controller는 drive line을 통해 이어져 있다.
3. 대부분의 LVADs는 continuous-flow mechanism을 통해 피를 공급하게 되고,
palpable한 pulse가 없으면서 normal mean arterial blood pressure가 유지되도록 한다.
4. Cardiac contractility가 조금 남아진(느껴지는) 환자에 있어서는 LVAD는 normal physiologic
cardiac output을 도와주도록(replace가 아닌) 한다.
5. Systemic perfusion이 minimal 한 cardiac function과 함께 남아있어, V-fib이 있는 와중에도
환자들은 stable 할 수 있다.
6. Clinical features
(1) Normal mean arterial pressures : 65~90mmHg
(2) ECG에서는 Discernible(확인 가능)한 QRS complex가 보인다고 한다. (Fiugre 2)
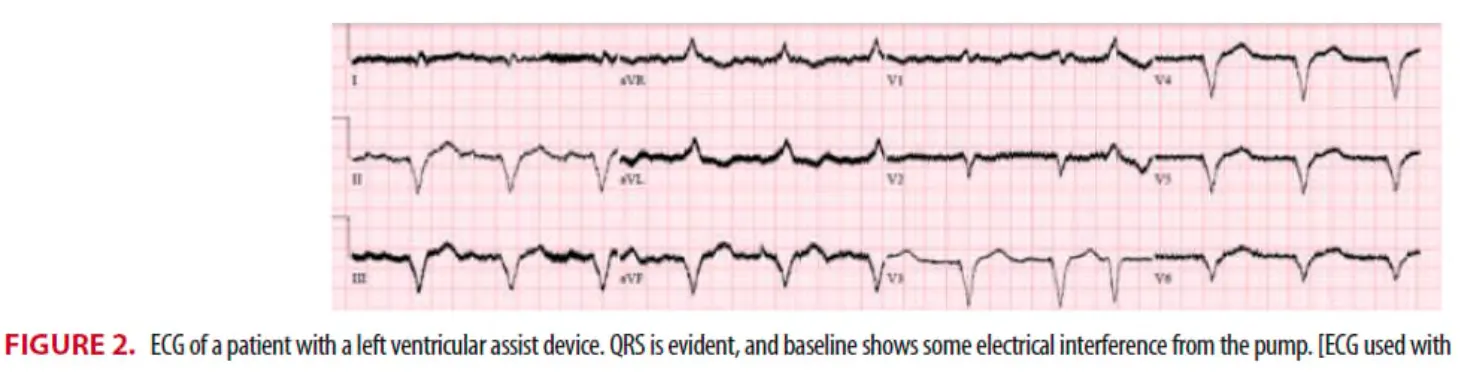
(3) LVAD는 chest x-ray에서 확인 가능하며, CT scan은 안전하나, MRI는 금기
7. The hemodynamically unstable LVAD patient
(1) LVAD 환자가 chest compression을 받는다면 LVAD가 heart와 aorta로부터 빠지게 될 것이며
LV rupture 등 야기할 수 있기 때문에 pump failure나 lack of perfusion test 등을 하는 것이
먼저라고 한다. (가능하면 안 해야 된다는 뜻)
(2) Pump failure or Lack of perfusion test 방법
1 Precrodium을 청진하여 whirr~ 하는 pump가 돌아가는 sound를 청진하는 것.
2 배터리 등을 갈아보는 것
3 Disconnect을 함부로 하지 말 것.
4 LVAD를 restart할 수 없다면, deep compression을 피하고 CPR을 조심스럽게 시작.
(3) Hypotension이 있는 환자에 있어서 normal saline을 loading하여 볼 수 있으며, 이에도 불구하고
hypotension이 지속될 경우 (fluid resusciation이 충분함에도), dopamine과 dobutamine과 같은
inotropics를 사용하라고 하고 있다.
(4) ECG를 통해 RV infarct이나 strain을 감별해야 함.
(5) Pulmonary embolism이나 device thrombosis가 있을 경우 heparin을 줄 수 있다.
(6) V-fib이나 Ventricular tachycardia가 unstable한 환자에서 있을 경우 defib 혹은 cardioversion을
ACLS guideline 따라 할 수 있으며, 다만 defibrillator pad를 drive line 위로 쓰지 말라고 하고 있다.
8. Medical한 complciation
Anemia / Bleeding / Thromboembolism
(1) Anemia : Can be caused by hemolysis (erythrocyte destruction from the pump)
(2) Bleeding and coagulopathy : INR target 2~3, bleeding은 standard한 방법으로 대처
(3) Infection : Sepsis가 의심된다면 그에 맞게 volume resuscitation, culture, anti 사용
2. Myocarditis (Inflammatory Cardiomyopathy)
(1) Pathophysiology
1 심근의 염증이 있는 상태
2 병리학적으로 focal infiltration of the pericardium by lymphocyte, plasma cells, histiocyte로
특징된다.
3 다양한 정도의 myocytolysis와 interstitial reticulin network의 파괴를 보인다.
4 많은 경우에서 mild하게 지나가기도 하고 pericarditis와 동반되기도 한다.
(2) Clinical features
1 Fever가 가장 흔히 동반되는 증상
2 증상은 myocardial involvement의 정도와 myocardial depression의 정도에 따라 다르게 나타남.
3 심한 경우 heart failure가 생길 수 있다.
4 Myocardial involvement가 적을 경우 systemic illness(fever, myalgia, headache) 등에 의해
myocardial dysfunction이 가려질 수 있다.
5 Retrosternal, precordial chest pain이 있을 수 있고 이것은 대부분 pericardial inflammation
(myopericarditis)로 인한 것이다.
(3) Diagnosis
1 Pericardial friction rub도 흔히 들릴 수 있다.
2 Chest x-ray : non-specific sign
3 ECG
: Nonspecific ST-T change를 보임
: Pericarditis가 동반될 경우 ST elevation, AV block, QRS prolongation을 보일 수 있다.
4 Cardiac enzyme이 증가될 수 있다.
5 Echocardiography는 비 특이적이다.
6 최근에는 nuclear imaging with positron emission tomography(PET)나 cardiac MRI 등 사용.
(4) Treatment and disposition
1 TOC : Supportive care, 대부분이 입원 치료가 필요함.
2 Rheumatic fever, diphtheria, meningococcemia와 동반될 경우 antibiotics가 필요
3 Immunosuppressive tx.가 특정 환자에서 이득이 있음이 있었으나 consistent한 도움 된다는 보고는
없었다.
C. Cardiomyopathies with diastolic dysfunction
C1. Hypertrophic cardiomyopathy
(1) Epidemiology and pathophysiology
1 최근에 정의되길, 다른 cardiac or systemic한 disease가 이러한 hypertrophy를 설명할 수 없는
상태를 말하며, non-dilated ventricular chamber는 특징으로 하는 unexplained LV hypertrophy의
상태를 의미한다.
2 Echo의 hall mark
: LV wall thickening (>15mm), or asymmetric septal hypertrophy & systolic anterior motion
3 유전 질환인 경우가 많다.
: Autosomal dominant inheritance를 보이나 sporadically 나타날 수 있다.
: 몇몇 particular genotype은 빠른 clinical course를 보일 수 있다.
: Benign genotype은 A.fib과 동반되어 stroke 등의 위험성이 있게 된다.
4 Hemodynamics
: LV의 hypertrophy → Reduced compliance → Abnormal LV syastolic function
( LV filling pressure가 증가한 것을 통해 알 수 있다 )
5 Cardiac output, Ejection Fraction, and end-systolic volumes은 대부분 정상.
6 대부분의 clinical symptom은 diastolic relaxation과 restricted LV filling 문제에 기한다.
(2) Clinical feature
1 DOE는 가장 흔한 증상이며 운동으로 인해 sinus tachycardia가 생기며 이로 인해 갑작스런
LV pressure의 증가, pulmonary venous hypertension이 생긴다.
2 추가적인 증상은 chest pain, palpitation, syncope가 있다.
3 흉통은 hypertrophy된 LV의 myocardial blood flow보다 산소의 demand가 많아져 발생하며
나이가 든 환자는 atherosclerotic coronary artery disease에 의해 perfusion 제한이 더 악화될 수
있다. 이 경우 NTG에 반응은 poor 하다고 함.
(3) Heart sound
1 첫 번째와 두 번째 심음은 일반적으로 정상이며, S4는 대부분의 환자에서 들린다.
2 Systolic ejection murmur가 환자의 left sternal border나 apex에서 흔히 들린다.
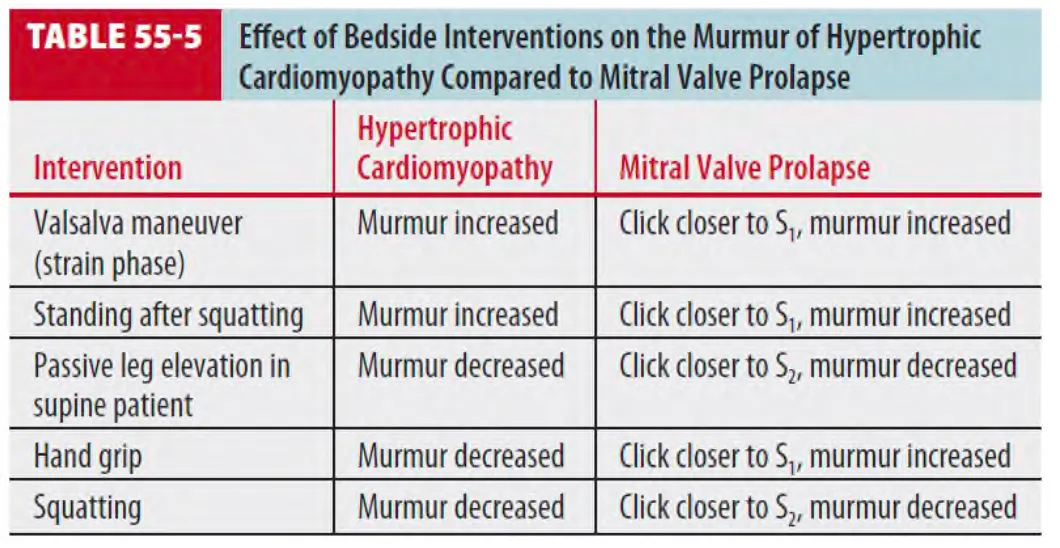
3 LV filling을 감소시키고 LV pressure를 떨어뜨리거나 심근 수축력을 증가시키는 경우
(ex. valsalva maneuver) murmur를 증가
4 LV filling을 증가시키는 경우 (squatting, passive leg elevation, hand grip) murmur를 감소
(4) Diagnosis
•
Resting ECG
◦
대부분 nonspecific하며 주로 LVH 및 LAE를 보인다.
◦
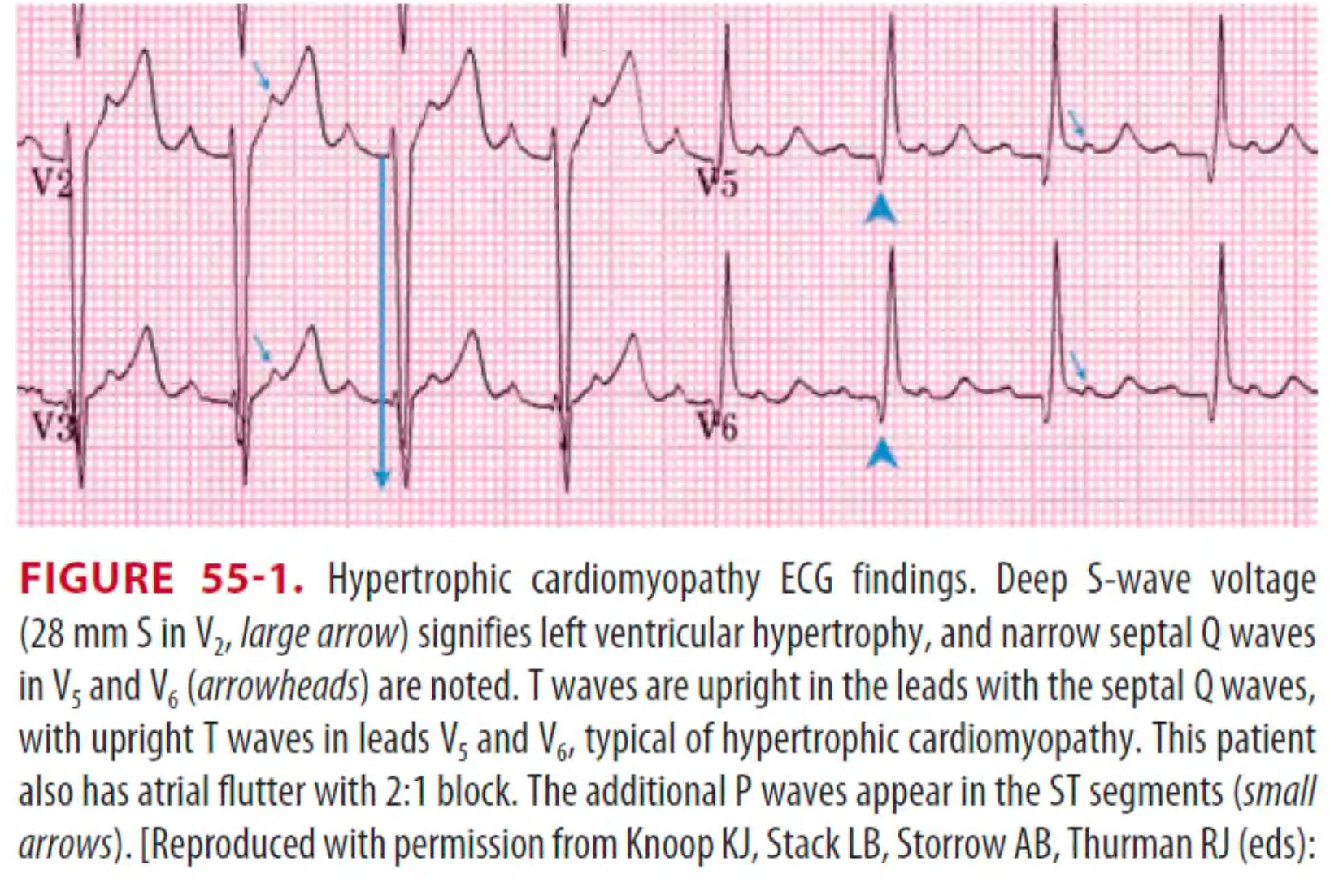
0.3 mv가 넘는 Q wave(septal q wave)가 anterior, lateral, inferior lead에 보일 수 있다.
(Dagger-like Q wave)
◦
Q wave를 MI에 의한 Q와 감별 : T wave의 polartity로 감별할 수 있다.
⇒ HCMP에서는 Upright T wave와 QS나 QR complex가 주로 보인다
반면, ischemic heart dz.에서는 T-wave inversion이 흔하다.
•
Echocardiography : 진단에 주요한 역할.
•
Cardiac MRI 등도 사용될 수 있다.
(5) Treatment and disposition
•
대부분의 환자들은 운동기능 저하, 흉통, 실신을 주소로 병원을 찾는다.
이런 경우 echocardiographic evaluation이 필요하다.
HCMP로 인한 실신이 의심될 경우 입원이 필요하다 (sudden cardiac death가 생길 수 있으므로)
•
그 외 extended ambulatory(Holter) monitoring, exercise stress test, tilt test가 필요하다.
•
폐부종 시 일반적 폐부종 치료 시행 (Vasodilator, Lasix, etc.)
•
β-blockers가 symptomatic patients 가 치료의 main-stay
: 비후성-유출로폐쇄성 심근병증은 Flow-limiting, Preload-dependent 한 상태
: Vasodilator 사용금기
: 심박수와 심근수축력을 줄여 flow gradient 를 줄이는 것이 중요함.
⇒ beta blocker 를 사용한다.
•
Shock 이 동반된 경우, Phenylephrine 40~100 mcg/min IV 하면 심근수축력 상승 없이 말초 혈관만 수축시켜 혈압을 올릴 수 있다.
C2. Restrictive cardiomyopathy
(1) Epidemiology and pathophysiology
1 대부분 idiopathic 하게 발생.
2 Myocardium의 replacement나 displacement를 야기하는 myocardium의 infiltration을 만드는
systemic disorder로부터 발생하기도 함.
(Amyloidosis / Sarcoidosis / Hemochromatosis / Progressive systemic sclerosis,
Carcionid heart disease / Endomyocardial fibrosis / Hypereosinophilic syndrome)
3 Restricted ventricular filling, normal or decreased diastolic volume을 특징으로 함.
4 Preserved ejection fraction이 있는 heart failure 환자에서 15% case가 restrictive.
5 Hemodynamic hallmark로 다음과 같은 3가지.
: LV and right ventricular end-diastolic pressure가 증가
: Normal LV systolic function (EF > 50%)
: Invasive한 hemodynamic assess를 할 때 발견되는 early diastolic ventricular pressure의 급격한
하강과 상승을 보이고 plateau를 보일때. (square-root sign, dip-and-plateau sign)
(2) Clinical features and diagnosis
1 Heart failure sign을 보임 (Dyspnea, Orthopnea, Pedal edema)
2 S3, S4가 들리며, pulmonary rales, jugular venous distention, Kussmaul sign, hepatomegaly,
pedal edema, ascites 있을 수 있음.
3 Chest x-ray : Normal or signs of heart failure
4 ECG
: Non-specific ST-T wave changes
: Cardiac conduction disturbances
: A. fib
: Low voltage QRS complexes
5 Differential diagnosis : Constrictive pericarditis or diastolic LV dysfuction
6 DOC
: Doppler echocardiography / Cardiac MRI
Cardiac catheterization with hemodynamic assessment
(3) Treatment and disposition
1 Constrictive pericarditis는 수술적 처치가 필요한 경우가 있기 때문에 둘을 구분하는 것이 중요하다.
2 치료 자체는 diurectics, ACEi 과 같은 symptom directed.
3 Sarcoidosis
: Corticosteroid therapy, hemochromatosis(chelation therapy) 등 가능.
: 대부분 입원 치료가 필요
IV. Pericardial Disease
1. Acute pericarditis
(1) Clinical features
1 가장 흔한 증상은 날카롭고 찌르는 듯한 precordial, retrosternal chest pain이다.
2 Pain은 갑작스러울 수도 있고 점진적일 수도 있으며, back, neck, left shoulder, arm으로 방사되며
inspiration이나 움직임으로 악화될 수 있다.
3 Left trapezial ridge refer pain이 동반될 수 있다.
4 일반적으로 흉통은 누워있을 때 심하고 앉거나 앞으로 기댈 경우 호전된다.
5 동반된 증상으로 fever, 통증 및 흡기 시 악화되는 통증으로 인한 dyspnea, posterior pericardium
에 의한 esophagus의 irritation으로 인한 dysphagia 등이 있다.
6 Pericardial friction rub
기댈 때 잘 들린다.
: 호흡 중 일부 시기에만 들릴 수도 있다.
: 가장 흔하고 중요한 소견이지만 시끄러운 응급실에서는 판단하기 어려울 수 있다.
: 청진기의 diaphragm으로 left lower sternal border나 apex에서 잘 들리며 환자가 앉거나 앞으로
: Pericardial friction rib은 triphasic하게 들리는 경우가 많으며 ventricular contraction에 의한
systolic component, early ventricle의 filling으로 인한 early diastolic component, atrial systole 에 의한 presystolic component로 나뉠 수 있다.
(2) Diagnosis
1 Serial ECG를 통해서 acute pericarditis를 진단할 수 있으며 4개의 stage로 나눌 수 있다.
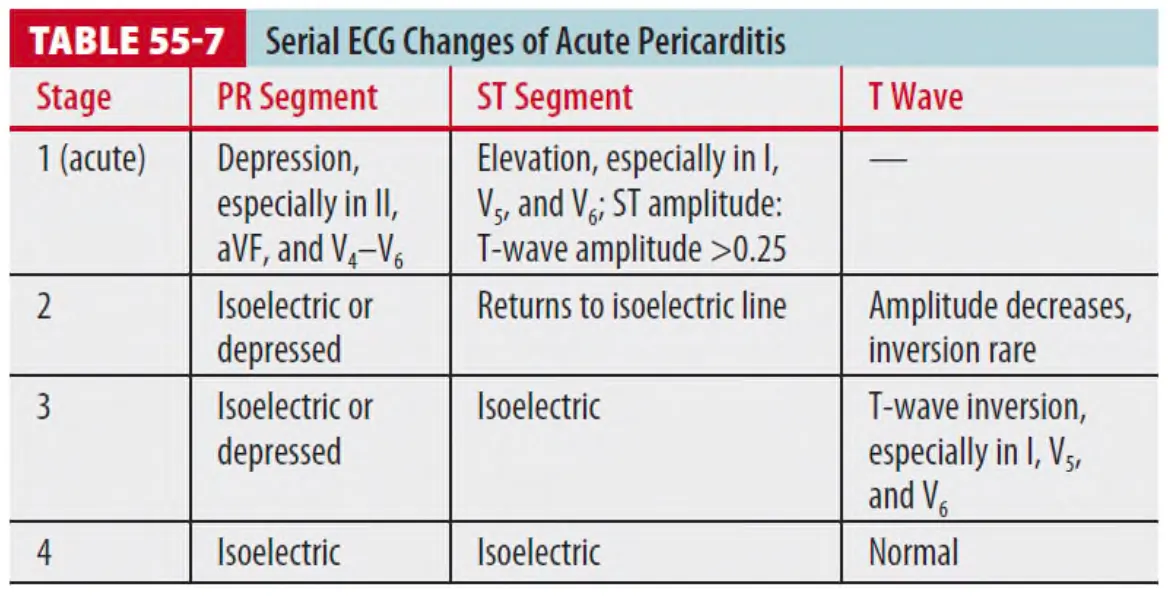
: 만약 많은 양의 pericardial effusion이 있다면 low voltage의 QRS complex와 electrical alternans를 보일 수 있다.
: Pericarditis와 early repolarization을 구분하는 것이 가장 흔한 문제이며, PR segment를 baseline 으로 하여 ST amplitude(mV) : T-wave amplitude(mV)가 >0.25 이상일 경우 acute pericarditis, <0.25일 경우 다른 early repolarization 가능성이 더 크다.
2 Echocardiography는 acute pericarditis와 pericardial effusion의 진단, 확진, serial f/u의 일차 검사이다.
(3) Treatment and disposition
1 Pericarditis는 대부분 idiopathic이나 viral로 1~2주 정도 증상이 지속되며,
이런 증상은 NSAIDs에 잘 반응하므로 7일에서 3주 정도의 NSAIDs 치료가 적절하다.
2 Corticosteroid를 NSAIDs를 쓰기 적절하지 않는 군에게 사용할 수 있으며,
Colchicine 0.5mg 경구 하루 두 번 투약이 재발이나 adjuvant therapy로 사용될 수 있다.
3 입원은 대부분 필요치 않다
4 Poor prognosis를 나타내는 indicator
: 38°C 이상의 발열 / 수 주 동안의 증상/ Immunosuppression / Oral anticoagulant의 사용
Myocarditis 동반 (elevated cardiac marker, CHF 증상) / Large pericardial effusion (>20mm)
5 일반적으로 이런 risk factor가 있는 환자나 chest x-ray 상 심비대를 보일 경우
빠른 echocardiography로 effusion의 양을 확인하고 serial 한 심기능 평가가 필요하다.
2. Nontraumatic cardiac tamponade
(1) Pathophysiology
1 Pericardial sac의 fluid의 증가는 intrapericardial pressure를 증가시킨다.
2 초기에는 pericardial volume-pressure curve는 flat 하지만 점차 fluid 양이 늘어나면서
intrapericarial pressure가 right heart의 normal filling pressure보다 커지게 되고
이로 인해 ventricular filling이 저하되는 cardiac tamponade 상태가 된다.
3 아래 요인에 따라 Cardiac tamponade가 발생
: Fluid accumulation의 속도
: Pericardial compliance (두꺼운 parietal pericardium일수록 덜 늘어난다)
: Intravascular volume (Hypovolemia시 ventricular filling pressure가 저하된다)
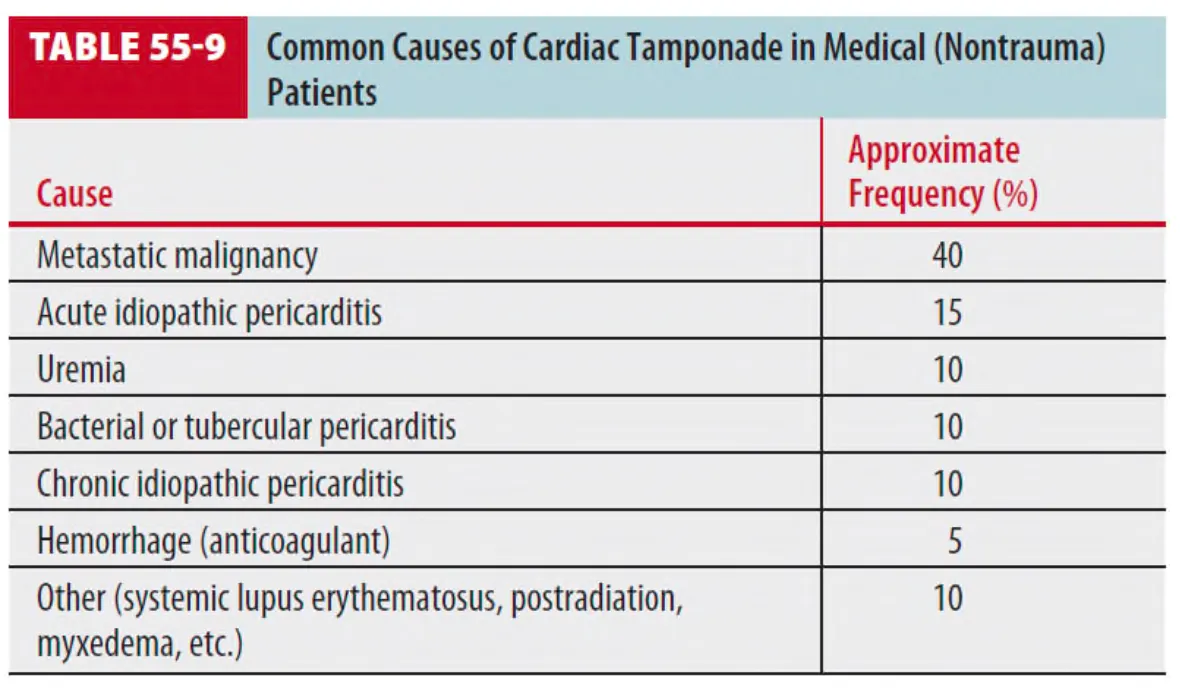
4 비외상성 cardiac tamponade의 원인으로는 metastatic malignancy가 가장 흔하다.
(2) Clinical feature and diagnosis
1 Symptoms : non-specific, dyspnoea를 가장 많이 호소
2 Pulsus paradoxus가 나타날 수 있는데 이는 흡기 시 수축기 혈압이 감소되는 현상으로
intrathoracic pressure의 변화가 심박출량에 영향을 미치는 상태이다.
3 일반적으로 systolic blood pressure가 inspiration 때 < 10mm Hg로 떨어지게 됨.
10mm Hg 이상으로 증가하게 될 때 true tamponade를 의심할 수 있음.
4 Neck vein distention이 absent “y“ descent와 함께 나타나며 apical impulse를 구별하기 어렵다.
5 심음은 멀리 들린다.(distant sound)
6 Chest x-ray
: Pericardial fluid 양에 따라 cardiac silhouette이 커져 보일 수도 있다.
7 ECG
: Low voltage QRS complex(<0.7mV)를 보임
: ST-segment elevation 및 PR-segment depression(epicardial inflammation으로 인해)을 보일
수 있다.
: Electrical alternans는 classic finding이지만 흔하지 않다.
8 진단은 clinical exam과 chest radiograph를 보고 의심!
9 Echocardiography가 진단의 DOC
: Large pericardial fluid volume과 함께 right atrial compression, RV diastolic collapse,
abnormal respiratory variation in tricuspid and mitral flow velocity, dilated inferior vena
cave with lack of inspiratory collapse를 보일 수 있다.
(3) Treatment and disposition
1 치료로 normal saline을 500~1000ml bolus로 주어 intravascular volume 증가, right heart filling을 촉진하여 cardiac output과 arterial pressure를 증가시킨다.
2 Hemodynamic instability를 보일 경우 pericardiocentesis를 응급실에서 시행할 수 있다.
