A. Empyema
A1. empyema의 흔한 원인균 (Table 66-1)
•
Pneumonia (m/c) : S.pneumoniae, S.aureus
•
Lung abscess / Aspiration pneumonia / Recent thoracotomy
: Mixed oropharyngeal anaerobes or S. aureus or G(-) bacilli
•
HIV환자에서 폐렴 : Tuberculosis, Fungal infection
•
Chest trauma : S.aureus or G(-) bacilli
•
Contiguous abdominal infection : G(-) bacilli, Anaerobes
•
Esophageal rupture : Mixed oropharyngeal anaerobes
Table 66-1 Empyema의 흔한 원인균 및 연관 질환
Pathology | Organism |
Pneumonia | Streptococcus pneumoniae, Staphylococcus aureus |
Pneumonia (Hib 백신을 맞지 않은 경우) | H. influenzae |
Lung abscess | Mixed oropharyngeal anaerobes |
Aspiration pneumonia | S. aureus |
Recent thoracotomy | Gram-negative bacilli |
Chest trauma | S. aureus, Gram-negative bacilli |
Contiguous abdominal infection | Gram-negative bacilli, Anaerobes |
Esophageal rupture | Mixed oropharyngeal organisms |
Postprocedure | Methicillin-resistant S. aureus, Pseudomonas |
Hospital-acquired empyema | Methicillin-resistant S. aureus, Pseudomonas |
Pneumonia in the setting of HIV | Tuberculosis, Fungal infections |
A2. Diagnosis
(1) Diagnostic criteria
: Thoracentesis를 통해 aspiration을 했을 때, pleural fluid 상성이 다음 중 하나 이상 시 empyema로 진단
1.
Gram stain or culture (+)
(참고로 gross puss거나 gram stain (+)인 pleural effusion의 경우 empyema로 진단,
Thoracostomy tube insertion을 한다.)
2.
Glucose <40 mg/dL
3.
pH<7.2 or LDH > 1,000 IU/L
•
TB에서 유래된 Empyema의 경우에는 Absolute lymphocyte count가 진단에 유용합니다.
(Interferon release assays 및 ADA도 유용합니다.)
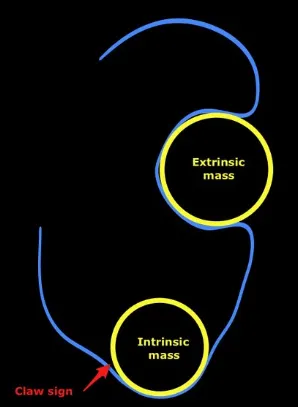
(2) CT 상 Empyema 와 Lung abscess 감별하기
•
인접한 Bronchi와 혈관들과의 관계
◦
abscess는 갑자기 Bronchovascular 구조물을 interrupt한다.
◦
empyema는 대개 인접한 폐를 변형 시키거나 압박한다
•
◦
empyema 는 visceral과 parietal pleura를 두껍게 만들면서 서로 분리시킨다
•
wall
◦
abscess는 두껍고 불규칙한 wall
◦
empyema는 대개 매끈한 walls
•
•
pleural enhancement
◦
empyema는 pleurar 가 enhance되는 경향
•
extrapleural fat
◦
empyema는 extrapleural fat의 부종과 haziness를 보이는 경향
A3. Treatment
•
폐렴이든 심부전이든 원인이 되는 기저 질환 치료.
•
Pain 조절은 NSAID 및 opioid
•
흉강천자 (thoracentesis) 는 호흡기 또는 심장 질환을 동반한 환자에게 도움을 줄 수 있으며,
호흡곤란의 증상 조절에 도움을 준다.
•
definitive 한 치료는 배액과 항생제이다. piperacillin-tazobactam 3.375-4.5g q6hrs IV 또는
imipenem 0.5-1.0g IV q6hrs 최근 병원에 입원해있었거나, invasive medicla device 삽입되어있
거나, 장기로 시설에 지내거나, 접촉 스포츠(contact sports), 비위생적인 집단 생활자, 동성애자
등 MRSA 위험군에는 vancomycin 추가.
•
삼출성 단계에서는 흉관 삽입과 항생제 병용.
•
섬유소성 화농성 단계에서는 흉강내 fibrinolytic agent 고려 및 흉부외과의 consult.
: Streptokinase, urokinase, 최근 deoxyribonuclease(DNase), alteplase 효과 보고됨.
•
혈흉 빈도를 낮추기 위해서는 tPA + DNase 함께 쓴다.
•
loculated 농흉시 비디오 흉강경 수술(Video-assisted thoracoscopic surgery, VATS)
•
조직화 단계에서는 fibrous peel 제거 위해 수술 고려.
(1) Pleuritic chest pain : NSAIDs or opioids
(2) Thoracentesis 적응증
•
환자가 respiratory or cardiac distress가 있을 때
•
Toxic patient에서 진단을 위해서
•
Esophageal rupture 등 life-threatening condition일 때
(3) Initial antibiotics (넷 중 하나 사용하면 된다.)
1.
Piperacillin-tazobactam
2.
Ampicillin-sulbactam
3.
a carbapenem
4.
Clindamycin
(4) PO Abx 로 변경
•
Drain + IV anti 치료 이후 임상적, 영상학적으로 호전 이면 경구 항생제로 변경
(5) Fibrinolytics
•
urokinase, alteplase, or streptokinase)의 사용이 Loculated된 Fluid collection의
Drainage에 도움이 됨.
A4. Empyema 의 치료에 영향을 주는 3가지 단계
(1) 삼출성 단계 (exudative)
•
발생 48시간 이내이며, effusion이 흐를 수 있는 상태.
•
흉관 삽입, 항생제만으로 해결 가능하다.
(2) 섬유소성 화농성 단계 (fibrinopurulent)
•
fibrin strand 생겨 loculation된 상태.
•
흉관만 가지고는 힘들다. 이 경우 intrapleural fibirnolytic agent 사용을 고려한다
•
VATS도 loculated empyema에서는 사용 가능하다.
(3) 조직화 단계 (organizational)
•
생기는데 수주가 걸리고, 섬유화가 심해진 상태로 "pleural peel"이 생겨서 폐의 팽창 장애까지 생긴다.
•
Fibrous peel을 제거하기 위한 수술적 치료도 고려한다.
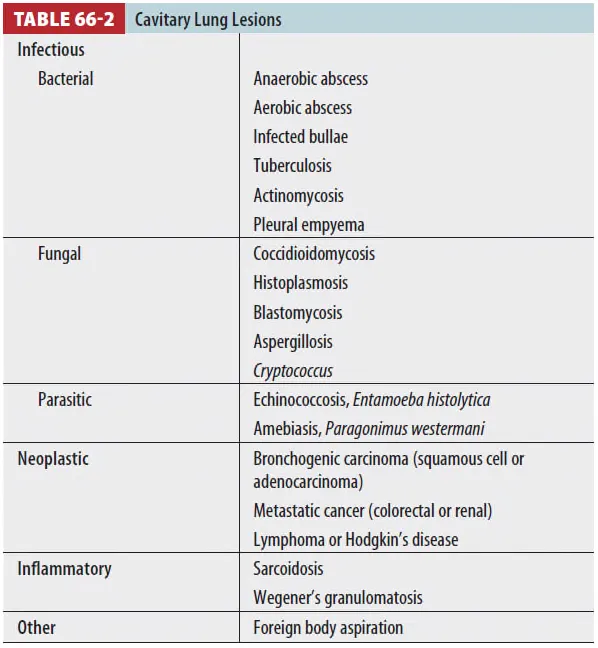
B. Lung abscess
B1. Pathophysiology
(1) M/C cause
① Aspiration pneumonia. 흡인 폐렴 시 약 7~14일 후 lung abscess가 호발
② 대부분 Anaerobic infection (Prevotella, etc)이 원인이며, Aerobic infection은 면역저하자에서
좀 더 흔함. (S. aureus, E .coli, Klebsiella, Pseudomonas, Streptococcus. etc)
(2) Primary lung abscess는 전체의 80%를 차지
① Good health people 및 aspiration에 취약한 자들에게 호발한다.
② Secondary lung abscess는 Malignancy 및 Immunocompression, extrapulmonary infection,
sepsis, surgery complication과 관련이 있으며 Mortality가 더 높다.
(3) Risk factors는 Aspiration risk와 상동.
(4) Lower lobe basal segment, upper lobe post segment에 호발.
B2. Diagnosis
(1) CXR : air fluid level이 이는 cavitary lesion이 관찰.
B3. Treatment
(1) Lung abscess는 70~90%에서 내과적 치료. 통은 tracheobronhial tree와 합쳐져 자연배출 됨.
(2) Antibiotics
① Ampicillin-sulbactam, 3 grams IV every 6 hours or Carbapenem (imipenem, meropenem).
•
8판까지는 Clindamycin이 drug of choice였으나 9판에는 C. diffile의 risk factor로 언급되며 another option으로 내려갔습니다.
Clindamycin + Cephalosporin is another option
(3) 내과적 치료에 반응하지 않는 경우 image-quided percutaneous drainage, thoracotomy, pulmonary resection 등을 고려
(4) 외과적 치료를 고려해야 하는 경우
① Poor outcome factor가 포함 ② Fungus,
③ Neoplasm ④ Parasite
⑤ Air-fluid level이 development 되는 경우
⑥ Critical hemoptysis나 empyema, bronchopleural fistula 등 complication이 동반된 경우
•
Poor outcome factors
: Aerobic infection / 고령 / Debilitation / Extrapulomary infection / 면역저하자
Malignancy / 영양결핍 / Sepsis.
B4. Disposition
(1) 환자의 증상이 resolution되고 나면 oral anti를 4~8주간 유지
(2) CXR findings은 대개 평균 2달 내 resolve