
•
Leptomeninges 의 염증으로, 치료하지 않은 세균성 뇌수막염은 100%의 사망률을 보인다.
•
바이러스성 뇌수막염은 다양한 중증도를 가지며, Herpes zoster 등 일부 바이러스에 의한 감염은 심한 감염을 일으킨다.
A. Epidemiology
1.
세균성 뇌수막염 (원인균은 연령에 따라 다르다)
(1) Neonate : Group B streptococcus, E. coli, Listeria monocytogenes
(2) Infants (>1month) : N. meningitides, S. pneumonia, H. Influenza
H. influenza Vaccination의 도입으로 H. influenza 유병률은 99% 감소
2.
바이러스성 뇌수막염
Enterovirus : 가장 흔한 원인
3.
진균성 뇌수막염 : Cryptococcus neoformans, Cocidiodies immitis, Candida albicans
B. Pathophysiology
1.
Common cause
: Bacteremia (Nasopharynx 에 colonize 되어있는 균에 의해 유발되는 경우가 대부분)
2.
Less common cause
: Direct spread from sinusitis, trauma site, dermal sinus tract 등
C. Clinical features
•
History
: Lethargy / Poor feeding / Fussiness / Bulging fontanelle / Vomiting / Diarrhea
Seizure / Grunting / Respiratory distress
•
Birth Hx
: Prematurity / LBW / Delivery complication / Maternal infection
Maternal group B streptococci / Herpes simplex
C1. Sign and symptom
(1) Bacterial meningitis
: Bulging fontanelle / 경부 강직 / 경련 / 섭취 감소 / 활동의 감소 / 갑작스런 shock
/ 의식 상태 변화 / 발열 / 두통 등
(2) Viral meningitis
: 보챔 / 활동의 감소 / 두통 / 발열
•
HSV는 심한 감염을 일으킬 수 있다.
Disseminated CNS involvement, Primary CNS ds, Skin lesion을 일으키며,
Neonate infection은 엄마의 Genital tract에서 감염되거나 다른 접촉으로 감염되어 발생 가능하다.
C2. Physical examination
•
90일 미만의 신생아와 영아에서 발열 외에도 정상체온 또는 저체온이 있을 수 있으므로,
정상 체온일지라도 뇌수막염을 배제할 수 없다.
•
1달 이내의 영아에서는 경부강직이 나타나지 않는 경우가 많다.
•
영아에서 38℃ 이상의 발열이(직장체온) 있는 경우 뇌수막염을 의심해봐야 한다.
•
90일 이상의 영아에서는 발열, 저체온, toxic appearance, lethargy, mottling, bulging fontanelle,
비정상적인 울음 등이 보일 수 있다.
•
36개월 이상의 유아, 소아에서는 발열, 경부강직, Kernig sign, Brudzinski sign등이 나타날 수 있다.
D. Diagnosis
D1. Lumbar puncture
(1) Lab 결과와 상관 없이 임상적으로 의심된다면 요추천자를 시행한다.
(2) Hypoxia, hypotension를 유발하거나 악화시킬 수 있다.
(3) 그 외에 thrombocytopenia, lumbar puncture site infection, vertebral abnormality 등에서 금기
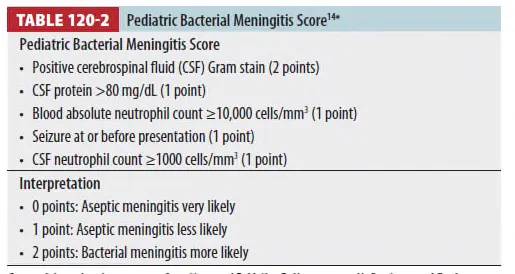
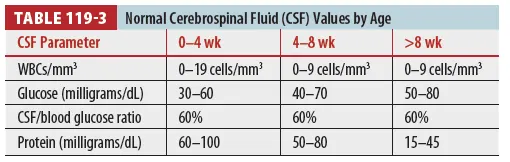
(4) CSF 검사에서 호중구 증가, Glucose 감소, Protein 증가가 관찰될 수 있다.
(5) PCR은 바이러스성 뇌수막염이나 결핵성 뇌수막염 감별에 도움이 된다.
E. Treatment
E1. Antibiotics
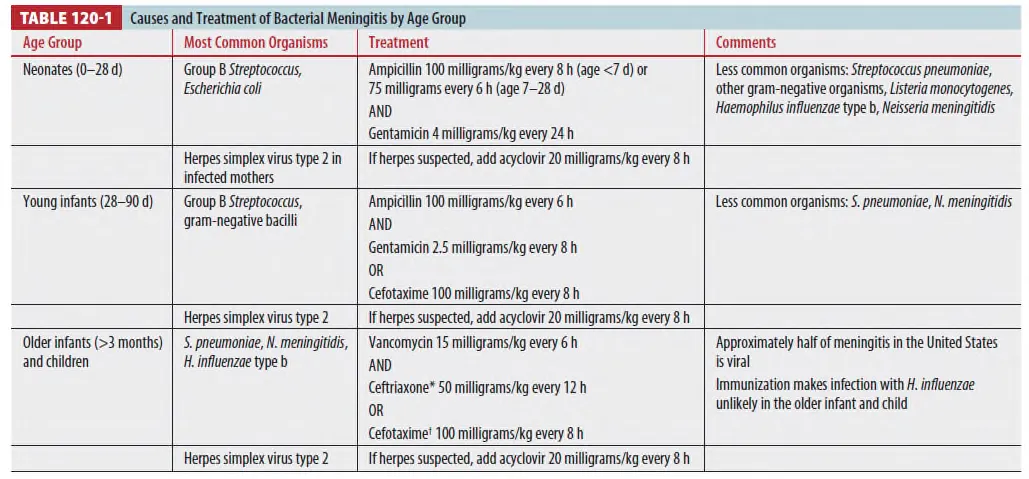
(1) Age에 따라 pathogen이 다르므로 Empirical treatement regimen이 다름 (Table 120-1)
(2) Neonate/Older infants/Children에서 HSV 감염 의심 시 IV Acyclovir 추가한다.
E2. Steriod treatment
(1) Inflammatory response에 의한 CNS damage(특히 hearing loss)를 줄이는 개념이나,
Benefit에 대해서는 논란이 있다.
(2) H. influenza type b에 의한 meningits에 사용에 고려해 볼 수 있으나 다른 bacterial
meningitis에는 추천되지 않는다.
→ 사용하는 경우 첫 번째 항생제 투여 이전에 쓰는 것이 가장 효과가 좋다.
F. Disease complication
1.
적절한 치료를 시행하면 Bacterial meningitis의 mortality는 10%로 감소
2.
Sensorineural hearing loss, Visual impairment, Sz, Hydrocephalus, Cognitive impairement,
Emotional problem 등의 sequale가 남을 수 있다.
G. Special consideration and special patients
G1. VP shunt infection
(1) Shunt 수술 후 바로 생기는 경우가 많음.
(2) Late infection의 경우 peritonitis, appendicitis 동반 가능성 높음
(3) 증상 : IICP 증상, shunt 주변 redness, swelling, 발열, 복통
(4) 치료 : Vancomycin + 3rd cephalosporin
(+ Aminoglycoside : Gram culture에서 gram(–) rod 확인 시)
G2. Unvaccinated child
(1) Septic 시 conservative manage 하며 LP → r/o meningitis
(2) Toxic appearance 없는데 fever focus 모호할 경우
→ WBC>15k 시 blood culture 하고 Ceftriaxone 주고 24시간 뒤 f/u
