
A. Electrical injury
A1. Introduction
•
High-voltage injury : 1,000V 이상
•
Low-voltage injury : 1,000V 미만
•
Electric arc flash burn
A2. Epidemiology
•
Incidence : 연간 6500건 (미국 기준), 대부분 업무 관련 (61%), Complication rate (10.6%)
•
Risk group : Power line worker (high voltage injury) / Electricians (arc burn) - m/c
A3. Basics of current flow
•
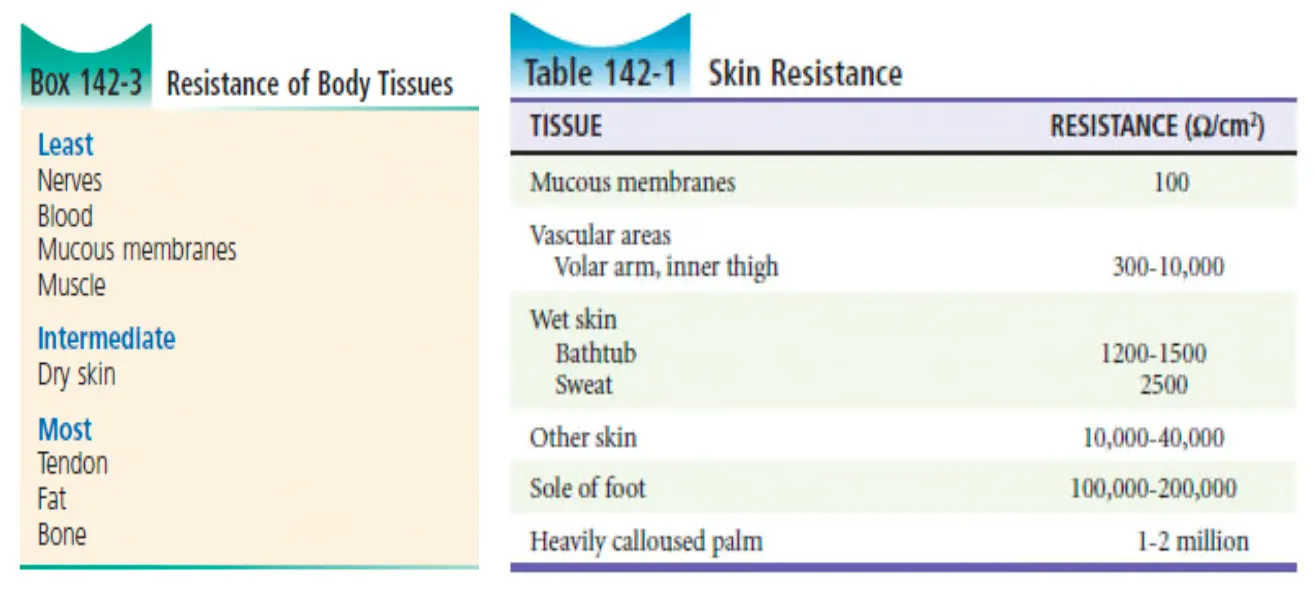
Fluid & electrolyte content를 많이 가진 조직이 그렇지 않은 조직보다 전기전도가 더 잘됨.
•
Bone은 가장 큰 resistance를 가진 생물학적 조직
•
Dry skin은 resistance가 높고 sweaty or wet skin은 resistance가 낮음.
•
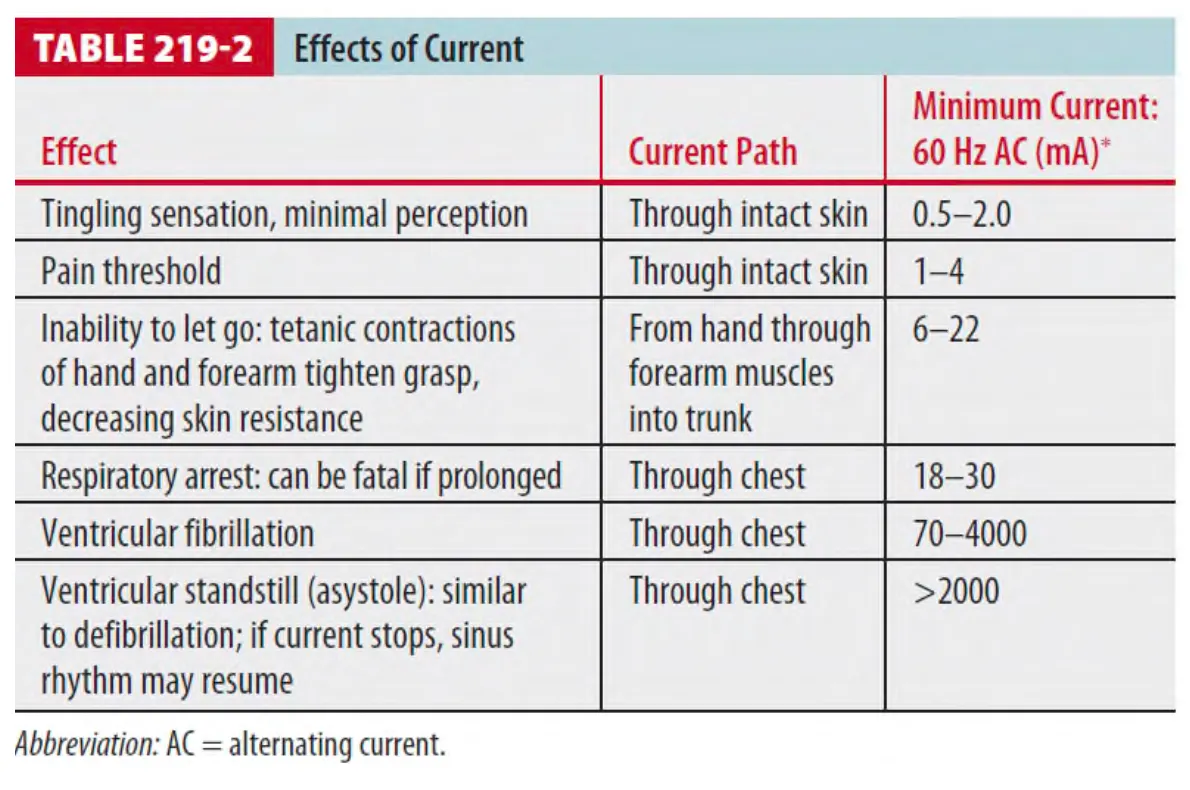
Electric shock의 생리적 효과는 amount / duration / type (AC or DC) / path of current flow 연관됨.
•
AC & DC
◦
AC : Standard household electricity / DC : Batteries and lightning is DC
1 교류파동 (Alternating current fluctuation)이 V. fib을 일으킬 수 있기 때문에 low-frequency (50~60Hz) AC는 비슷한 레벨의 DC보다 더 위험할 수 있음.
◦
AC current는 muscular tetany 일으킬 수 있고, 이는 electrical source에서 피할 수 없게 할 수
있음.
◦
AC, DC current 둘 다 희생자를 current source에서 멀리 떨쳐지게 할 수 있고, 이는 severe
blunt force injury를 야기할 수 있음.
•
몸을 통해 흐르는 전류 흐름의 패턴은 어느 몸부위의 손상이 있을지를 판단하는데 사용될 수 있음.
A4. Mechanisms of electrical injury
(1) High- & Low-voltage injuries
•
Voltage에 따라 serious & fatal electrical injury 의 risk가 증가 (특히, 600V 이상에서)
•
High voltage : Defined as >1000V
◦
Severe musculoskeletal, visceral, and nervous system injury와 관련
via 전기에너지로부터 직접적인 손상
◦
발열로 인한 조직손상
◦
mechanical injury from trauma induced by a fall or muscle contraction.
(2) Electrical burns
•
High voltage : 심각함.
•
Low voltage : 열에너지가 적어서 화상은 흔치 않음
(3) Electric Arc Injuries
•
아크 방전 : 가스 및 전극 물질의 증기 속에 전압을 가하면 전류가 흐름 → 아크가 발생
•
화상이나 10feet 밖의 사람을 죽일 수 있을 정도로 충분하게 열을 내뿜음
•
사람을 던져버릴 정도의 폭발 발생
•
일반적으로 수천 volt에서 발생 → 섭씨 2만도 까지 온도가 상승.
•
Arc에서 방사된 열 자체와 옷에 불이 붙어서 화상을 입을 수 있음.
(4) Tetanic Contractions
•
지속적인 근위축 및 경련 유발 가능.
•
Type (AC or DC), frequency, voltage, 접촉범위에 따라 효과가 다름.
•
AC current through forearm : Flexor tetany of fingers and forearm
•
강제적인 근위축이 골절이나 탈골을 유발 가능함. (especially, around shoulders)
•
손이나 손가락이 전도체를 꽉 쥐게 되면, 전도체에서 벗어나지 못하며 지속적으로 낮은 저항 수준의 접촉이 지속될 수 있음.
•
전도체 접촉이 지속될 경우, 시간이 지남에 따라 heat-related damage가 축적되며, tight한 grasp이 지속되면 resistance가 낮아져서 손상 정도가 점점 심해짐 (deep tissue에 damage 늘어남.)
•
몸통과 다리를 통하는 지속적인 전류 : Opisthotonic posturing (활모양 강직) 일으킬 수 있음.
→ 추가적인 기계적 손상 발생 가능
A5. Clinical features of electical injury
(1) 발생 가능한 임상적 특징
•
즉각적인 부정맥 발생
•
호흡정지 (호흡부전)
•
경련
* 흉부를 horizontally or vertically transverse 하는 전류는 부정맥/호흡 부전 등을 일으킬 수 있음.
(2) Cardiac injury
•
응급실 도착 전, Asystole / V. fib으로 사망 가능성이 있음.
•
Low voltage injury < 1,000V
: 무증상, 정상 EKG를 가진 환자는 더이상 evaluation 할 필요 없음.(이후 부정맥 유발하지 않는다.)
: 혈관손상 (Spasm, Thrombosis, Dissection)에 의한 심근손상 가능, 전도장애 발생 가능.
(3) CNS and spinal cord injury
•
신경학적 문제 - High-voltage injuries의 약 50%에서 발생
•
Brain Injury
: 일시적인 LOC는 흔함
: Focal neurologic deficit 발생 가능.
(Agitation, confusion, coma, seizures, quadriplegia, hemiplegia, aphasia, visual
disturbances, blindness)
: Head, cervical spine CT - Rule out traumatic etiologies
: MRI - Purely electrical damage가 있는지 확인하기 위하여 필요
•
Spinal Cord Injury
: 8% of high-voltage electrical injuries
: 척추골절, 순수한 전기적 손상, 혈관손상에 의해 발생 가능.
: Initial MRI finding - 영구적인 손상에도 불구하고 MRI는 정상으로 나타날 수 있음.
: Newer MRI imaging protocol - Standard MRI에서 놓친 abnormalities 발견할 수 있음.
•
Delayed spinal cord dysfunction
Progressive vascular injury (특히, spinal artery) or delayed cell membrane damage
(축적된 free radical 효과)에 의함 → Progressive demyelination 유발.
(4) Peripheral nerve injury
•
둔감증 (Paresthesias) : Immediate / Transient / Delayed (up to 2 years)
•
Extensive peripheral nerve damage : Minimal thermal injury로부터 유발 가능
•
Median or ulnar neuropathy
: 손바닥에 전기적 접촉이 있을 때 radial nerve injury보다 흔하게 온다.
: 그러나 지속적인 증상이 있더라도 nerve conduction study는 이상이 없을 수 있음.
(5) Cutaneous burns
•
전기와 접촉한 부분에 발생함
•
DC 직류전류 : Entry and exit wounds
•
AC 교류전류 : Contact wounds
•
화상 전문 입원 치료가 필요한 경우 : Painless, grey to yellow, depressed areas
(6) Orthopedic injury
•
2가지 원인 : 경직성 근육 위축 / 동반된 추락
•
Wrist, forearm, humerus, femoral necks, shoulder, scapula은 Trauma 없이도 집에서 쓰는 전기용량으로 골절이 발생 가능. (120~220V AC)
•
Posterior shoulder dislocation이 흔함.
(7) Vascular and muscle injury
•
High-voltage injury에서 가장 흔하다
•
Early spasm과 delayed thrombosis, stenosis, aneurysm 유발
* High-voltage
: 1초 미만의 짧은 접촉(or arcing)에도, compartment syndome 발생의 risk가 높음
: Contact with >1000V로 인하여 발생한 아래와 같은 심각한 문제들
- Prehospital cardiac arrest, crush injury, compartment syndrome나 수술이 필요할 정도의
전 피부층에 걸친 skin burns들이 있다면, tissue damage에 의한 body fluids의 빠른 손실과 연관
: Requiring aggressive resuscitation
(8) Coagulation disorders
•
Thermal injury or tissue necrosis는 coagulation disorders를 유발가능
•
Low-grade DIC, transient coagulopathies, unmask underlying vascular injury
(ischemic stoke)
(9) Blast injury
•
Electric arcs : 다른 폭발과 비슷한 정도의 강한 strong blast pressure가 발생 가능.
•
Blast와 연관된 mechanical trauma에 의한 Brain injury, blast와 연관된 alveolar disruption에 의한 arterial air emboli 발생 가능.
(10) Inhalation injury
1 Chemical toxins (e.g. ozone) : Coronas or arcs 등에 의하여서 생성 가능함.
2 Ozone
: Mucous membrane에 불편감을 주고, 일시적인 호흡기능 장애, 폐출혈 및 폐부종 유발 가능함.
3 화재 및 폭발에 의한 CO의 흡입이나, 다른 toxic substance에 의한 중독도 가능함.
(11) Ocular injury
•
Cataract : 수주, 수년 뒤에도 발생할 수 있다.
•
Corneal injury, retinal detachment, uveitis, intraocular hemorrhage/thrombosis, optic nerve damage
(12) Auditory Injury
•
Auditory system : Damaged by current or by hemorrhage in the tympanic membrane,
middle ear, cochlea, cochlear duct, and vestibular apparatus.
•
Delayed complications : Mastoiditis, Sinus thrombosis, Meningitis, and brain abscess.
•
위와 같이 발생한 complication에 의하여 즉시 혹은 늦게라도 hearling loss가 발생할 수 있고, 불편감이 있다면 formal f/u 함.
(13) GI injury
: Bowel perforation / Intra-abdominal hemorrhage
A6. Scene and prehospital care
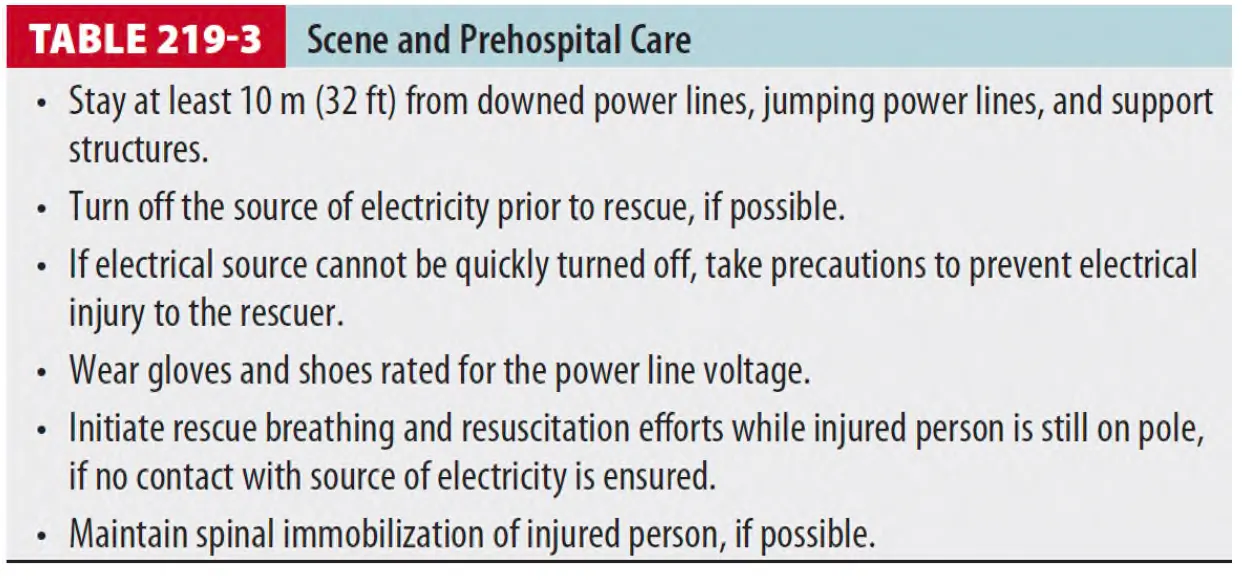
(1) 600V 이상에서는, 마른 나무 및 그 외 물질도 전도가 가능하기 때문에 구조용을 사용해선 안됨.
(2) Scene resusciation and stabilization
•
Low-voltage AC는 V. fib을 유발 가능.
•
High-voltage AC and DC은 주로 transient ventricular asystole을 유발
A7. ED diagnosis and treatment
•
일반적인 ABC (airway, breathing, circulation) 및 major trauma와 같은 resuscitation 시행
•
Spinal immobilization은 유지되어야 함
•
Cardiac arrhythmias : ALS guidelines에 맞추어 resuscitation 진행.
•
ED cardiac monitoring : High-voltage injuries & 증상이 있는 모든 환자
•
Cardiac complications
: More common in high-voltage injuries / with LOC /Ventricular & atrial / dysrhythmias / bradydysrhythmias / QT-interval prolongation
•
증상이 없고 EKG가 정상인, low-voltage의 손상을 받은 환자 : 입원 필요 없음
(1) P/Ex
•
조직 손상 및 그와 동반된 합병증을 찾아낸다
•
조심스럽게 혈관 및 신경학적 검사를 시행
•
Initial assessment에서의 정상 소견이더라도 심각한 손상이나, delayed spinal cord injury를 배제하지 못함.
(2) ED evaluation
: should next focus on systematic assessment and treatment
•
혈액 및 영상학적 검사 of high-voltage injuries : Trauma guidelines을 따름
•
Low-voltage injuries : 환자가 무증상, 신체진찰 이상 없다면 lab & image 검사 필요 없음
(3) Fluid resusciation
•
Parkland formula (4 mL/kg x percentage of body surface area burned, for 24 hours)에
의거
•
Fluid는 Parkland formula and physical examination으로 추정되는 것보다 더 필요할 수 있음.
(4) Myoglobinuria
•
For monitoring of compartmend SD, rhabomyolysis, AKI
•
Urine output 1~2ml/kg/hr 이상 유지.
•
Correction and prevention of electrolyte abnormalities
•
24시간 이내에 fasciotomy가 필요한 예후 인자 (3가지 중 1개 이상)
(1) Myoglobinuria
(2) 전신의 20% 이상의 화상
(3) 전신 12% 이상에서의 full-thickness burn
A8. Disposition and follow-up
(1) Low-Voltage Injuries (600V 미만)
•
Asymptomatic + ≤240 V AC + Normal ECG/PEx → 귀가 가능
•
Feel unwell or have any new ECG abnormality → Monitoring 및 재평가
•
Symptoms beyond superficial skin injury or abnormal lab/ECG
→ May have systemic injury & admission 필요
(2) High-Voltage Injuries (600V 이상)
•
≥ 600V AC, 명백한 손상이 없더라도 observation을 위해 입원치료 필요!
•
Asymptomatic + Normal ECG : Routine cardiac monitoring이 필요하진 않음.
A9. Special populations
(1) Pregnant women
: IUP 20~24wks – Fetal heart rate & uterine activity 적어도 4시간 이상 monitoring 필요
(2) Children
•
Oral and Lip Burns
•
Unilateral, involving the lateral commissure, tongue, and/or alveolar ridge
•
Systemic complications : 흔치않음
•
입술동맥의 손상
: 즉각적으로 드러나지는 않음.
: Severe bleeding up to 10% (after 5 days)
: Bleeding may occur up to 2 weeks after injury
(3) Hand Wounds
: 다른 injury나 신경학적 증상 없다고 판단되면 discharged after local wound care
