
A. Thrombophilia
A1. Introduction
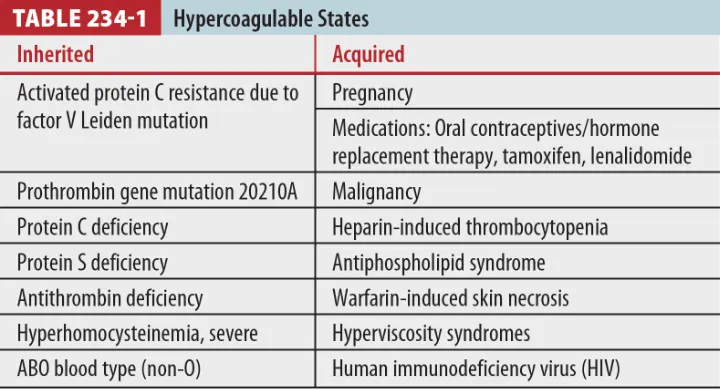
(1) Arterial or venous thrombosis의 다양한 원인 (Table 234-1)
(2) Local factors (ex. focal atherosclerotic lesion in coronary artery disease) 및 major systemic events (ex, 외상, 수술, prolonged immobilization), 유전적 요인 등이 관련
A2. Pathophysiology
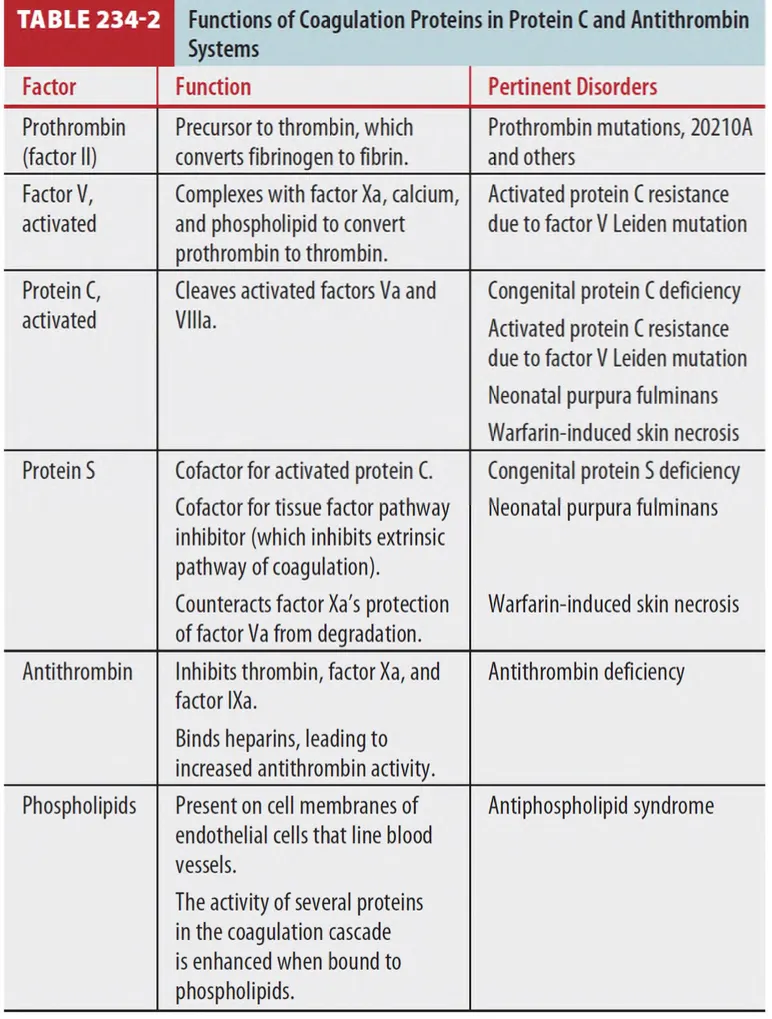
* 두가지 주요 항 혈전 pathway : Antithrombin, protein C (Table 234-2)
(1) Antithrombin
•
Activated coagulation factor(주로 thrombin, factor Xa, IXa)를 억제한다.
•
Heparin은 antithrombin 작용을 증진시켜 anticoagulant activity를 나타낸다.
(2) Protein C
•
Vit. K-dependent protein으로 endothelial cell surface에 결합하고 thrombin에 의해 활성화되어 factor Va, VIIIa를 쪼갠다.
•
Protein S 역시 Vit K-dependent protein으로 위 기전의 cofactor로 작용
A3. Diagnosis
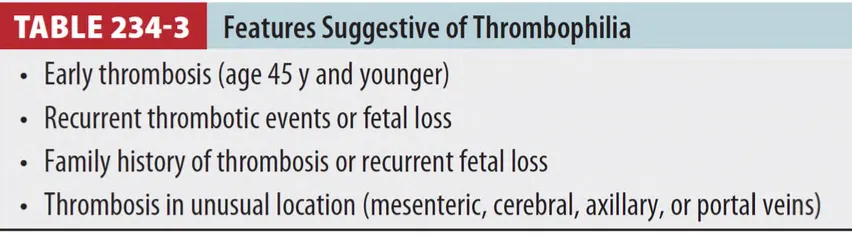
(1) Thrombophilic 질환은 응급실에서 진단은 드물다. thrombophilia가 있는 환자에서 혈전증의 high risk를 인지하고 과응고 상태를 의심할 수 있는 적절한 진단적 정보를 얻는 것이 중요 (Table 234-3)
(2) 응급실 환경에서는 lab 결과로 hypercoagulable condition 여부를 파악하기 힘들며, Vit. K antagonist(와파린) 복용 및 급성 혈전증의 경우엔 일부 factor level 값을 신뢰할 수 없음.
(3) ED에서는 thrombophilia를 의심하고 적절한 평가의뢰 및 acute thrombosis의 처치가 중요
(4) Hypercoagulable disorder 환자에서는 D-dimer 수치가 정상이어도 venous thromboembolism을 배제할 수 없다.
A4. Treatment and disposition
(1) 현재 항응고요법 하지 않는 환자는 고위험 상황 (ex. 수술, 임신과 산후기, 장기여행)에서 예방적으로 항응고제를 복용하는 것을 고려해야 한다.
(2) 에스트로겐 기반의 피임약이나 호르몬 치료는 피해야한다.
A. Specific conditions associated with thrombophilia
A1. Inhertied clotting disorders
(1) Activated protein C resistance (Factor V Leiden mutation)
•
가장 흔한 inherited hypercoagulable disorder
•
Factor V 유전자의 single point mutation, factor Va가 protein C 작용에 저항성을 갖게 되어 Prothrombin → Thrombin 과잉 전환
•
PTE보다는 DVT와 매우 큰 관련, 임신 중 preeclampsia, 태반 파열, fetal growth restriction, 사산 초래
(2) Prothrombin gene mutation
•
Prothrombin 생합성이 증가되어 hypercoagulable state 유발됨
•
Venous thromboembolism과 임신 합병증이 증가
(3) Antithrombin deficiency
•
Antithrombin gene에 several mutation이 발생
•
Type 1 (수 저하), type 2 (기능 저하)
•
임신 합병증, venous thrombotic event
(4) Protein C & S deficiency
•
Protein C or S 수적 감소 혹은 기능 저하
•
Warfarin-induced skin necrosis의 위험이 높음.
: Warfarin이 protein C, S의 합성을 억제
: 예방 위해서는 와파린을 loading dose로 쓰지 말고, 적정 INR에 도달할 때까지 heparin 유지
(5) Hyperhomocysteinemia
•
Homocysteine 대사에 관여하는 효소의 기능 저하 (혈중 homocysteine은 증가)
•
Arterial, venous thrombosis 위험 증가
A2. Acquired clotting disorders
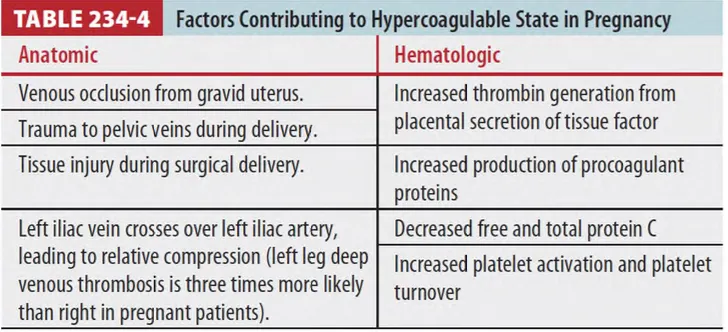
(1) Pregnancy and estrogen use (Table 234-4)
•
임신 중 coagulation의 변화는 출산 과정에서의 과다출혈을 예방하기 위한 적응
•
High estrogen state로 혈전 생성 경향 커짐.
•
피임약 장기복용자, hormone replacement 치료 중인 경우에서도 나타날 수 있다.
•
Estrogen
: Procoagulant proteins (factor VII, VIII, X, prothrombin, fibrinogen) 증가
: Anticoagulant proteins (antithrombin, protein C, S) 감소
(2) Malignancy
•
암환자에서는 thrombus 생성위험이 증가 (특히 췌장, 뇌, AML, 위, 식도, 산과, 신장, 폐암)
•
Arterial thrombotic event도 증가시킴 (Ex. MI, Ischemic stroke)
•
항암치료 자체도 protein C, S를 down-regulation시킴으로써 coagulation에 영향
•
Active cancer 환자에서 venous thromboembolism이 발생하면 LMWH을 6개월 유지,
보행 가능한 환자에서 예방적인 anticoagulation은 추천되지 않음
(3) Heparin-induced thrombocytopenia
•
Consumptive coagulopathy로 arterial & venous thrombus 생성
•
헤파린 치료 시작한지 5~15일경 발생하며 Plt 50k~60k/mm3로 감소
•
Plt factor 4 (heparin을 중화하는 역할)가 주요역할을 한다.
: 헤파린-PLT factor 4 Ab complex가 PLT에 결합
→ clot을 만듦으로써 plt 수 감소
→ 이 complex는 endothelial cell, monocyte를 자극
→ Tissue factor를 분비하게 해서 coagulation cascade를 더욱 촉진함
•
의심 시 헤파린(unfractionated, LMWH 모두) 중단
•
Warfarin은 일시적인 protein C 결핍으로 인한 microvascular thrombosis 위험이 있기 때문에
heparin-induced thrombocytopenia 초기에 warfarin 사용은 피해야 한다.
(4) Warfarin-induced skin necrosis
•
Warfarin은 Vit. K-dependent coagulation factor의 생성을 억제
•
Warfarin 투여를 시작하면 protein C가 procoagulant protein보다 먼저 감소하며, 일시적으로 hypercoagulability 상태가 된다.
•
Extremities, breast, trunk, penis에 발생, painful central erythematous macule
→ Localized edema → Purpuric zone → Necrosis
•
Warfarin loading dose 사용은 피하고, thrombin inhibitor(LMWH)으로 시작해야 함
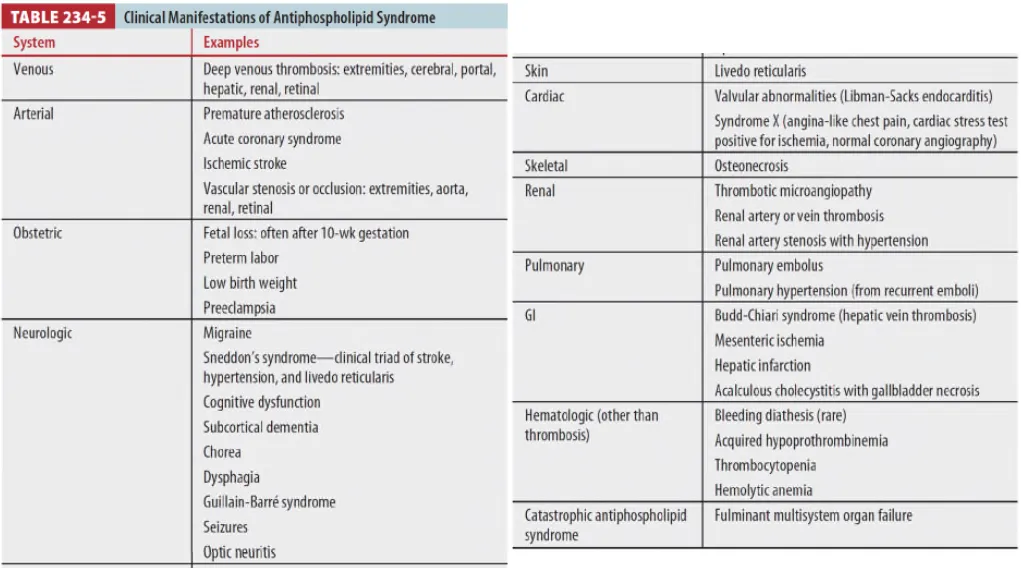
(5) Antiphospholipid syndrome (APS) (Table 234-5)
•
Antiphospholipid antibody 가 있는 상태에서 정맥/동맥의 혈전과 임신 중 이상이 발생하는 질병
•
APS에서 발견된 항체는 protein C, S, prothrombin을 타겟으로 함
•
APS 환자는 대부분 다른 원인이 없지만 (primary), 자가면역질환 (SLE), 감염, 약물 (phenytoin, hydralazine, cocaine)등의 선행 요인이 있는 경우도 있다 (secondary)
•
Thrombotic event가 재발하는 APS 환자는 평생 anticoagulation이 필요함
•
임신한 APS 환자는 heparin이나 저용량 아스피린 유지
(6) Hypercoagulability associated with other disorders
•
Nephrotic syndrome
: Anticoagulant protein의 배설 증가, endothelial injury 및 plt aggregation 증가를 유발함
•
Vasculitis (Behcet’s syndrome, syndrome, antineutrophil cytoplasmic antibodyassociated
vasculitis, granulomatosis with polyangiitis)
•
Hyperviscosity syndrome (essential thrombocythemia, polycythemia vera, Waldenstrom’s
macroglobulinemia, multiple myeloma,and sickle cell disease)
•
Smoking, DM, HIV
