
chromextension://efaidnbmnnnibpcajpcglclefindmkaj/https://synapse.koreamed.org/upload/synapsedata/pdfdata/0119jkma/jkma-50-1096.pdf
•
Primary PPH
- 자연분만 시 500 cc 이상
- C/sec 시 1,000 cc 이상 출혈
•
Secondary PPH
- 분만 24시간에서 6주 내에 상당한 양의 출혈이 있는 것.
A. General Consideration
•
혈액 500cc 마다 Hct 3% 씩 감소
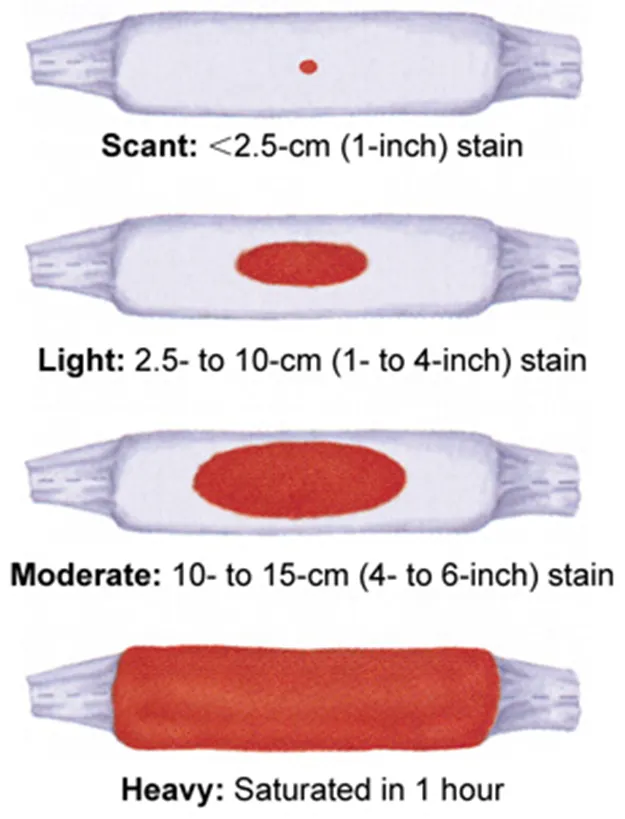
A1. 출혈량 추정
•
4*8 거즈 한 장 : 약 10 mL
•
패드 한 뼘 * 한 뼘 : 약 200 mL
•
무게 1g = 1mL
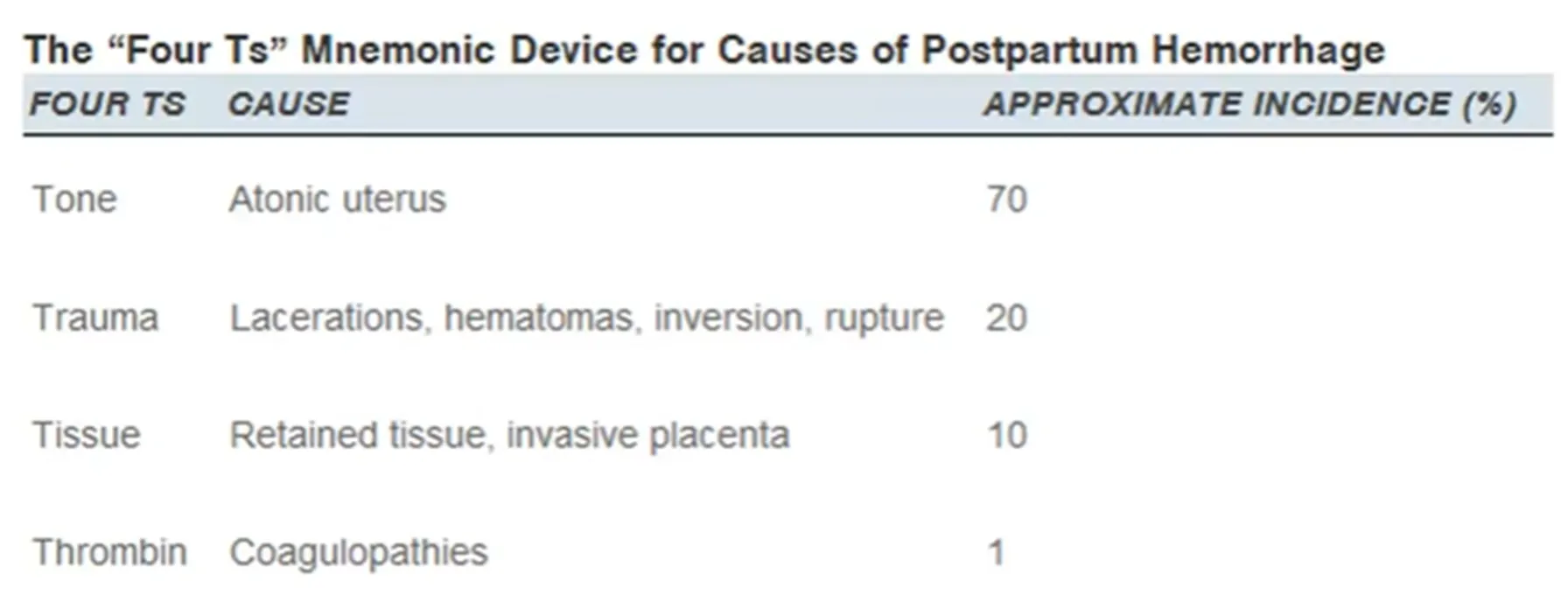
A2. 원인
•
Uterine atony
•
Genital tract laceration
•
Vulvar, vaginal hematoma
B. Uterine Atony
•
분만 후 자궁이 적절한 수준으로 수축하지 못해 태반이 부착된 부분의 혈관에서부터 출혈이 발생
B1. Risk factor
•
Primiparity and high parity
•
Oversitended uterus woth a large fetus, multiple fetus, hydramnios
•
Labor abnormalities
•
Labor induction with PG or oxytocin
•
Prior postpartum hemorrhage
(1) 예방적 옥시토신 투여 ⇒ 위험도 60% 정도 감소
•
Oxytocin 10 U IM
◦
5 U IV bolus
◦
10~20 U/L N/S IV at 100~150 mL/hr
B2. Evaluation and management
•
Laceration과 만출된 태반 확인
•
지속적인 fundal massage and uterotonic agent
(1) A & B
•
10~15 L/mmin O2 by face mask
(2) C
•
2 large bore IV access
•
Sampling for Lab, Crossmatch 4 PRBC
•
2L of crystalloid rapidly
•
Transfusion ASAP
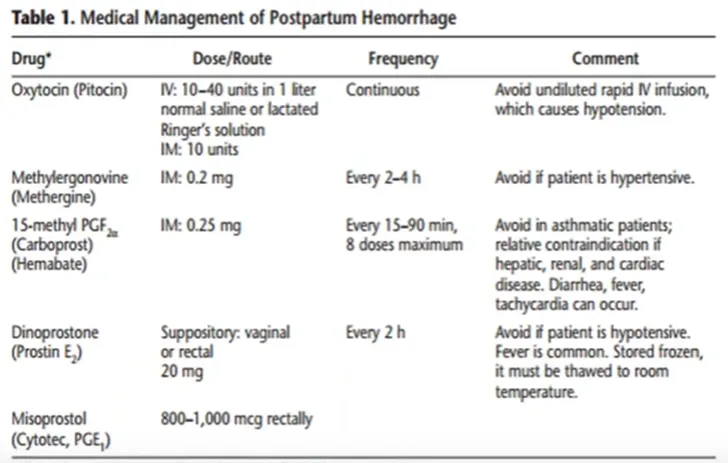
(3) Uterotonic agent
: 분만 후 출혈의 예방 및 치료
•
Oxytocin (IV, IM 사이에 우위는 없다)
•
Ergot alkaloid : 2nd line (Methergine, ergonovine 0.2 mg IM)
: oxytocin과 병용투여 가능
•
Prostaglandin E & F
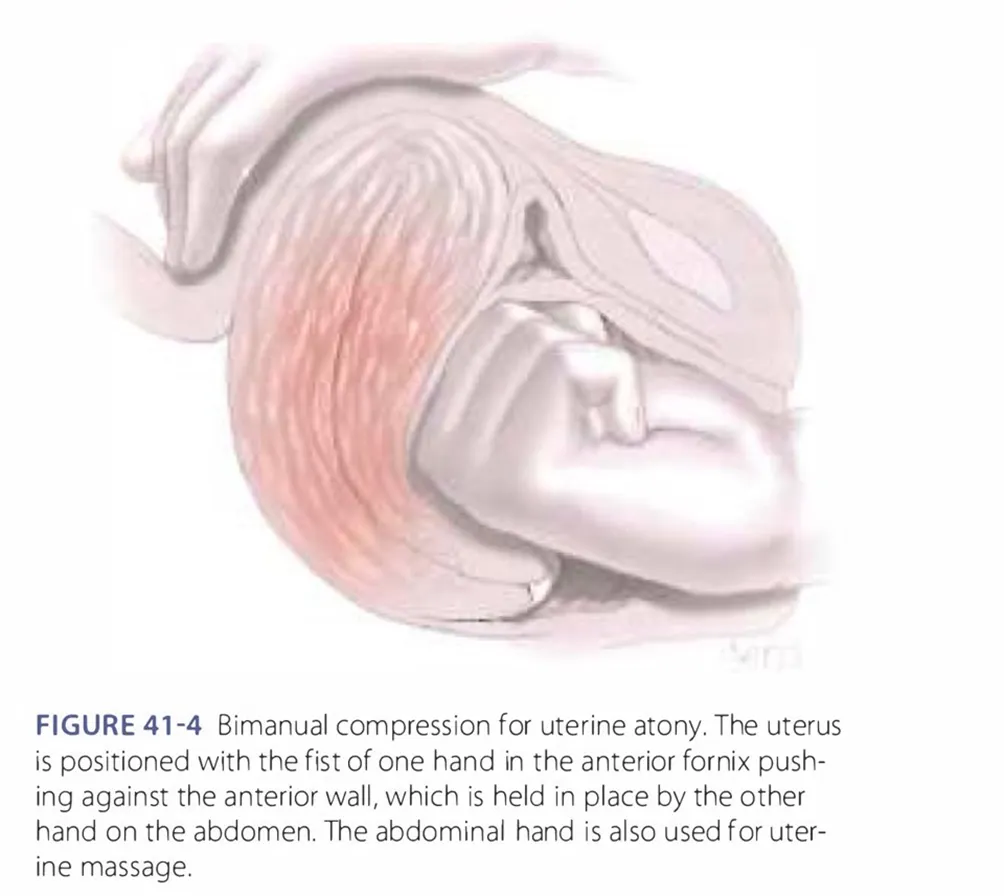
(4) Uterotonic agent에 반응하지 않는 출혈
•
Bimanual uterine compression
•
2 IV line - oxytocin, transfusion
•
Uine output check
•
Crystalloid rapid infusion
•
마취 후 remnant placenta나 uterine rupture, laceration 여부를 손으로 확인
•
Cervix와 vagina에 laceration이 생겼는지 육안 확인
•
여전히 불안정할 경우 Transfusion
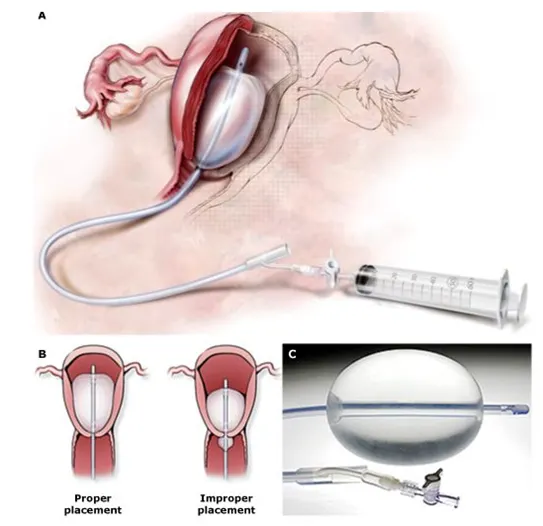
(5) Bakri
(6) Surgical procedure
•
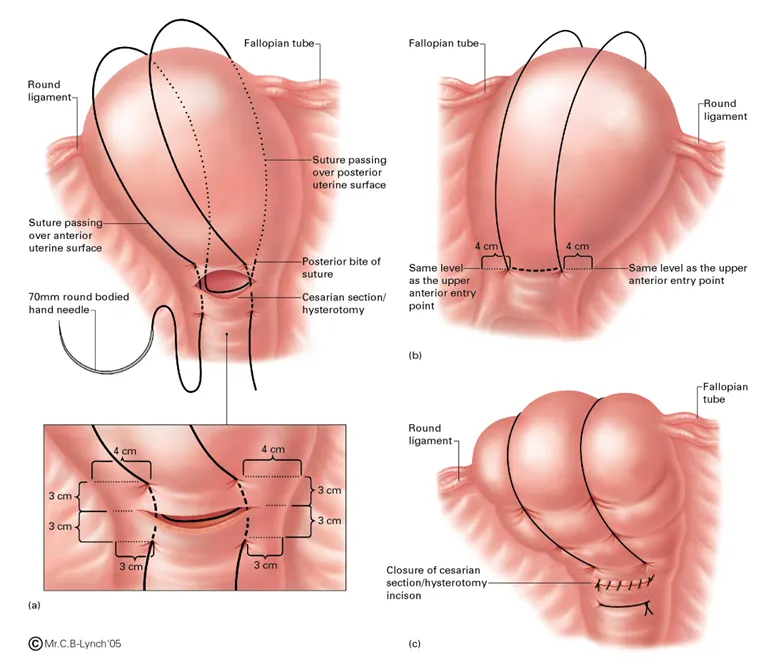
uterine compression suture
•
pelvic vessel ligation
•
angiographic embolization
•
hysterectomy
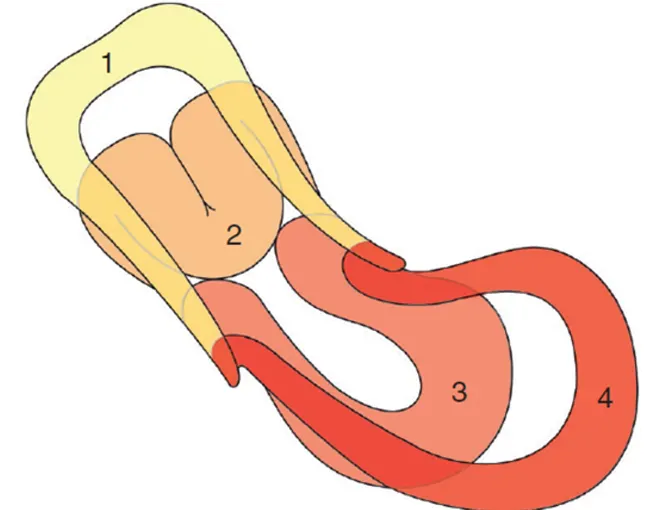
C. Uterine Inversion
•
즉시 정복하지 않으면 심한 출혈 및 pain shock 가능함.
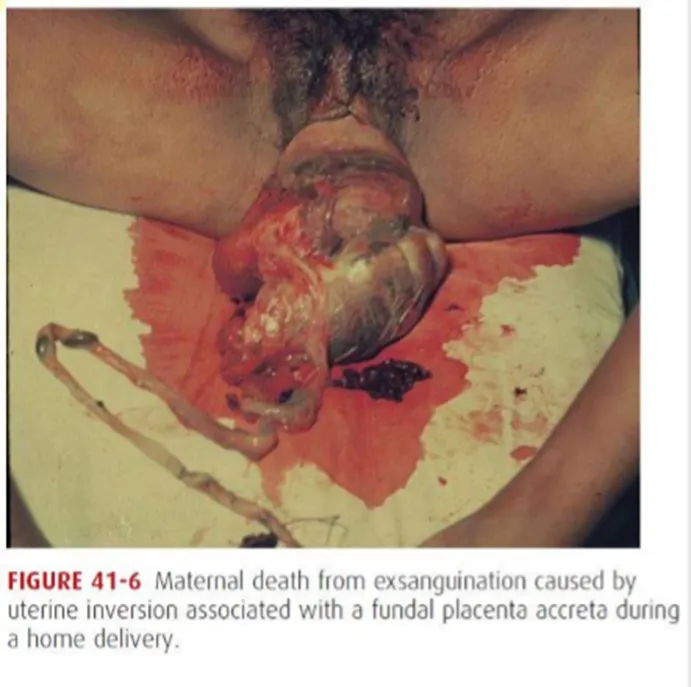
C1. Risk factor
•
Fundal placental implantation
•
Uterine atony
•
Cord traction before placental seperation
•
Abnormaly adhered placentation with accrete syndrome
C2. Recognition and management
: 빠른 진단이 매우 중요함
(1) 태반이 이미 분리되었다면 - 자궁을 push up하면 종종 정복이 된다.

(2) 태반이 분리되지 않았다면
•
자궁의 relaxation 및 repositioning을 위해 tocolytics처방이 권장.
(3) Surgical intervention
