

https://www.youtube.com/watch?v=zfWKcTixM6E : LBP P/Ex 동영상
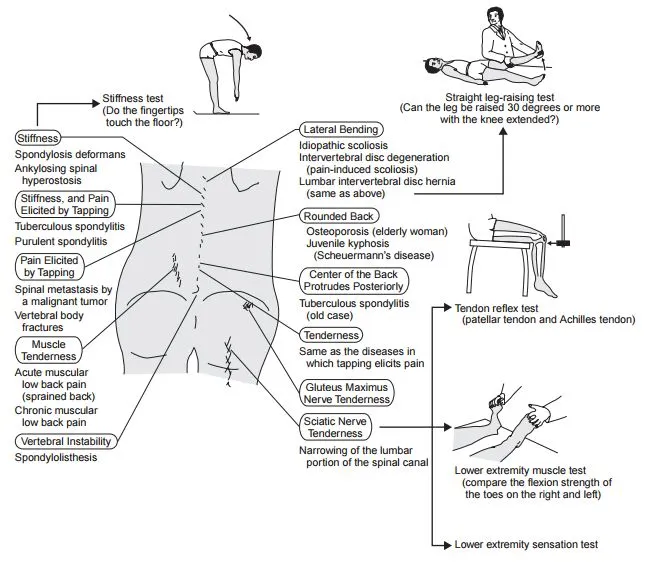
A. Straight Leg Raising Test (SLRT; Laseque test)
•
각 다리를 개별적으로 약 70도까지 들어올림.
0~35 도 : No dural movement
35~70 도 : Sciatic root에 tension이 가해진다
70도 이상 : 통증은 대부분 관절 통증이다
•
Herniated disc의 스크리닝 검사 : 68~80% sensitive for a L4-5 or L5-S1 herniated disc
•
양성반응은 60도 이하에서 무릎 아래쪽으로 방사통이 유발됨
•
통증이 유발되면 다리를 좀 내리고 발목을 dorsiflexion하거나 머리를 최대한 들어올린다.
•
두 가지 중 한 동작에서 양성이라도 Radiculopathy나 척수종양일 수 있음.
•
Contralateral SLRT양성 : HLD가 크고 Protrusion 또는 Sequestration일 수 있음.

B. Neri's test
•
Radiculopathy나 척수종양 의미 ??
B1. 시행방법
1.
똑바로 선다
2.
허리를 구부려 발가락을 손가락으로 터치하게 한다
3.
무릎이 구부러지는지 확인한다
B2. Positive Neri’s Sign
•
척추가 flexion되면서 다리 통증과 함께 무릎이 굽혀짐
•
Nerve root compression
•
SI/lumbar sprain/strain
•
hamstring contracture

C. Femoral Stretch test : Reverse SLRT
•
엎드린 상태로 한 쪽 무릎을 90도 구부리고 무릎을 들어올린다.
•
양성 - 동측 Ant. thigh에 통증
양성은 L3, L4 nerve root가 문제 있다는 것.
•
대부분의 HLD는 L5-S1 nerve root를 involve
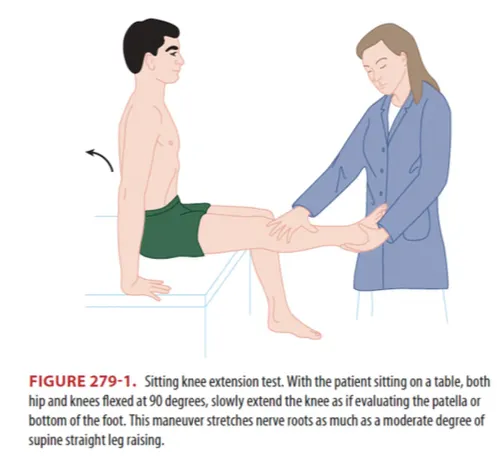
D. Sitting knee extension test
•
SLRT 과 같은 원리로 nerve root stretching 시켜서 통증 유발되는지 보는 검사.
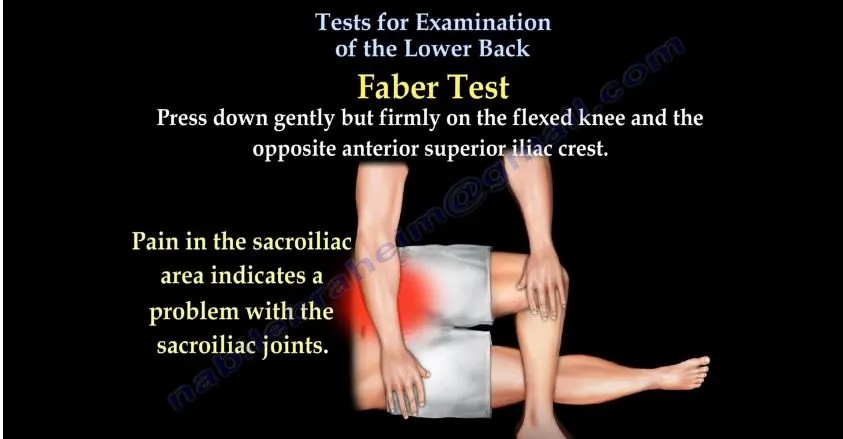
E. Faber test
•
SI joint의 문제를 파악하는 방법
•
SI joint 부분에 통증 유발되면 SI joint 문제
•
확진검사는 아님
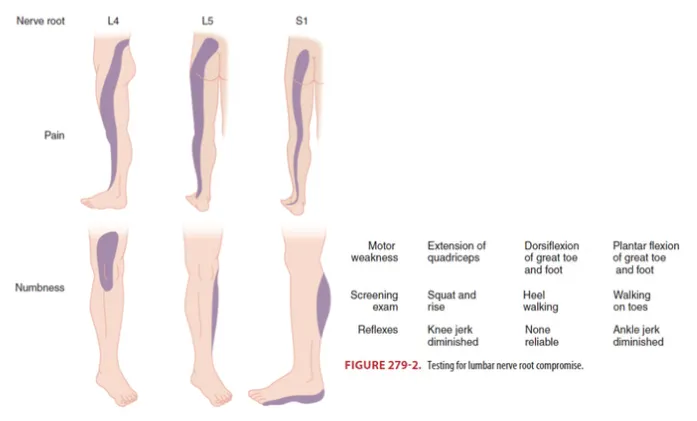
F. Disc hernation m/c site
1. L5 nerve root : L4~L5에서 눌린 후 L5~S1으로 나온다 → 종아리 바깥쪽 저림감
2. S1 nerve root : L5~S1에서 눌린 후 S1~S2으로 나온다 → 종아리 뒤쪽, 발바닥 저림감
3. 치료 : 3~6주 동안 대증 치료 (호전 없으면 수술 고려)
G. Myelopathic sign
•
Ankle Clonus, Barbinski sign
H. Spinal stenosis (척추관 협착증)
•
Spinal canal, nerve root canal, intervertebral foramina 포함한 lumbar spine narrowing
•
걸을 때 발생하는 low back pain, lower extremity pain, claudication (절뚝거림)
•
휴식이나 앞으로 구부리는 자세에 의해 통증 호전된다
I. Epidural compression syndrome
•
Spinal cord compression, Cauda equina syndrome, Conus medullaris syndrome을
총칭하는 용어
•
Complete epidural compression 진단은 가능하지만, 조기 증상과 징후로 진단하는 것이 어려움
•
하지 쇠약 및 감각변화, 자율신경장애를 유발하는 대부분의 질환들이 초기 감별진단에 포함
→ Hx taking과 physical exam으로 다른 질환과 spinal cord 또는 cauda equina의 compression
lesion을 감별해야 한다.
•
Nontraumatic epidural compression
◦
Spinal canal hemorrhage with hematoma
◦
Tumors of the spine or epidural space
◦
Spinal canal infections including spinal epidural abscess
◦
Transverse myelitis
◦
Massive midline disk herniation는 비압박성 질환이지만, spinal cord compression과 임상 양상이 비슷하다.
I1. Clinical features
(1) History
•
Back pain with associated neurologic deficits
: Perianal sensory loss
: Fecal incontinence or urinary incontinence with or without retention
: 한쪽 또는 양쪽 다리 좌골 신경통 (Sciatica)
•
증상 지속기간으로 감별하기 어렵다.
•
Urinary retention > 500ml
± 3개 중 2개 (양측 좌골 신경통, Subjective urinary retention, rectal incontinence)
→ MRI로 확인된 cauda compression의 가장 중요한 예측인자
•
Malignancy 병력과 신경학적 증상, 특히 양측 증상 급속한 진행은 compression 가능성이 높다.
(2) Physical exam
•
Compression level과 compression 면적에 따라 신체검사가 다르다.
•
Cauda equina syndrome
: 가장 흔한 소견은 Urinary retention ± Overflow incontinence (민감도 90%, 특이도 95%)
•
하지 쇠약 및 강직, 감각 이상 또는 감각 결손, 보행 곤란 및 SLR test 이상
: 가장 흔한 sensory deficit은 Buttocks, Posterosuperior thighs, perineal region
→ 일반적으로 saddle anesthesia라고 한다.
•
Anal sphincter tone은 60~80% 정도까지 감소
I2. Diagnosis & management
•
종양으로 인한 경막외 압박이 의심되는 경우에는 확진 검사 전 10mg IV dexamethasone 주사
→ 주사 후 Spine MRI with gadolinium 시행 (Spine 전체 MRI 시행)
•
Disk herniation으로 인한 Pure cauda equina syndrome이 의심되면 Lumbosacral MRI 시행
•
종양의 경막 외 압박에 대한 임상적 결과는 환자 증상에 따라 다르며, 치료 전 걸을 수 없는 환자는
치료 후에도 대부분 걸을 수 없다.
: 너무 약해서 도움 없이 걸을 수 없는 하반신 마비가 아닌 환자의 50% 정도가 다시 걸을 수 있다.
: 치료 시작할 때 걸을 수 있는 사람들은 보행 상태를 대부분 유지한다.
•
치료 전 urinary catheter가 필요한 환자 중 82%가 치료 후에도 계속 필요하다.
•
MRI 소견 상 Tumor로 cord compression 소견 있으면 Spine surgeon urgent consultation
→ Decompression and/or radiation therapy

